

Benefits and Risks of Clopidogrel vs. Aspirin Monotherapy after Recent Ischemic Stroke: A Systematic Review and Meta-Analysis
- PMID: 31867054
- PMCID: PMC6913341
- DOI: 10.1155/2019/1607181
Benefits and Risks of Clopidogrel vs. Aspirin Monotherapy after Recent Ischemic Stroke: A Systematic Review and Meta-Analysis
Abstract
Aim: Though combination of clopidogrel added to aspirin has been compared to aspirin alone in patients with stroke or transient ischemic attack, limited data exists on the relative efficacy and safety between clopidogrel and aspirin monotherapy in patients with a recent ischemic stroke. We aimed to compare clopidogrel versus aspirin monotherapy in this population.
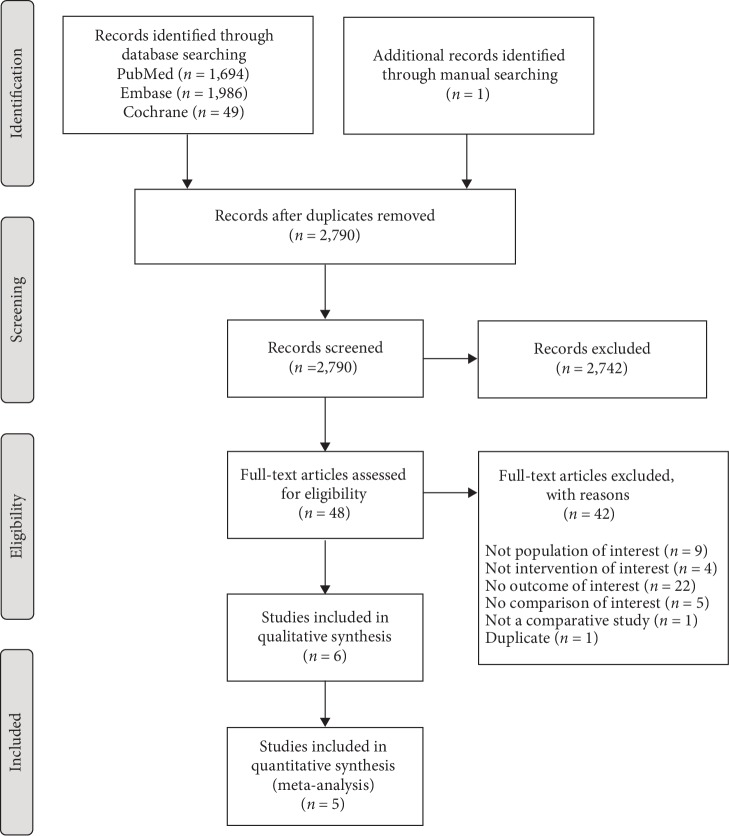
Methods: PubMed, Embase, and CENTRAL databases were searched from inception to May 2018 to identify clinical trials and observational studies comparing clopidogrel versus aspirin for secondary prevention in patients with recent ischemic stroke within 12 months. Pooled effect estimates were calculated using a random effects model and were reported as risk ratios with 95% confidence intervals.
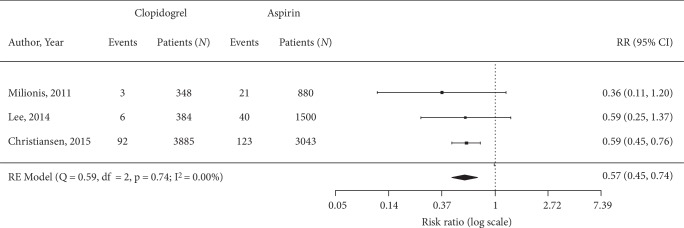
Results: Five studies meeting eligibility criteria were included in the analysis. A total of 29,357 adult patients who had recent ischemic stroke received either clopidogrel (n = 14, 293) or aspirin (n = 15, 064) for secondary prevention. Pairwise meta-analysis showed a statistically significant risk reduction in the occurrence of major adverse cardiovascular and cerebrovascular events (risk ratio 0.72 [95% CI, 0.53-0.97]), any ischemic or hemorrhagic stroke (0.76 [0.58, 0.99), and recurrent ischemic stroke (0.72 [0.55, 0.94]) in patients who received clopidogrel versus aspirin. The risk of bleeding was also lower for clopidogrel versus aspirin (0.57 [0.45, 0.74]). There was no difference in the rate of all-cause mortality between the two groups.
Conclusions: The analysis showed lower risks of major adverse cardiovascular or cerebrovascular events, recurrent stroke, and bleeding events for clopidogrel monotherapy compared to aspirin. These findings support clinical benefit for single antiplatelet therapy with clopidogrel over aspirin for secondary prevention in patients with recent ischemic stroke.
Copyright © 2019 Maurizio Paciaroni et al.
Conflict of interest statement
Maurizio Paciaroni received honoraria as a member of the speaker bureau of Aspen, Sanofi-Aventis, Boehringer Ingelheim, Bayer, Bristol Meyer Squibb, Daiiki Sankyo and Pfizer. Birsen Ince has received honoraria from Pfizer and Sanofi-Aventis within the past 36 months, outside the submitted work. Kursad Kutluk has received honoraria from Boehringer Ingelheim, Pfizer and Sanofi-Aventis within the past 36 months, outside the submitted work. Dara Paek, Jung Min Han, and Michael del Aguila report employment by Doctor Evidence at the time in which this research was conducted, who was contracted by Sanofi to perform the analysis. Shalini Girotra reports employment by Sanofi. All other authors have nothing to disclose.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
