

Remote Tool-Based Adjudication for Grading Diabetic Retinopathy
- PMID: 31867141
- PMCID: PMC6922270
- DOI: 10.1167/tvst.8.6.40
Remote Tool-Based Adjudication for Grading Diabetic Retinopathy
Abstract
Purpose: To present and evaluate a remote, tool-based system and structured grading rubric for adjudicating image-based diabetic retinopathy (DR) grades.
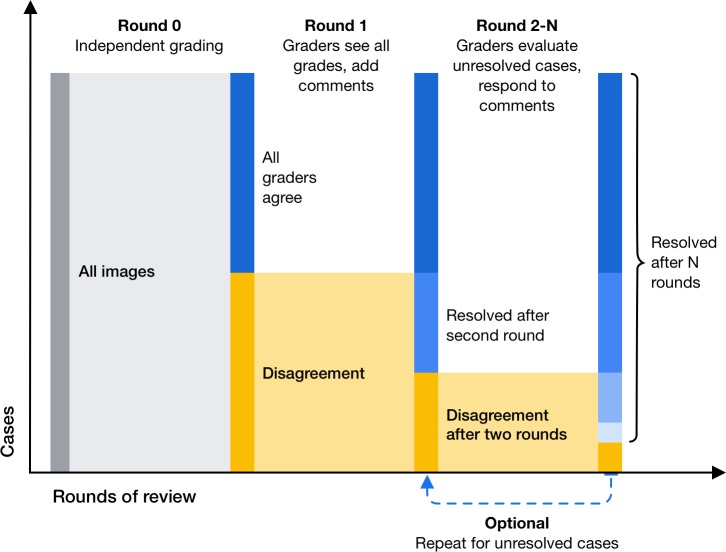
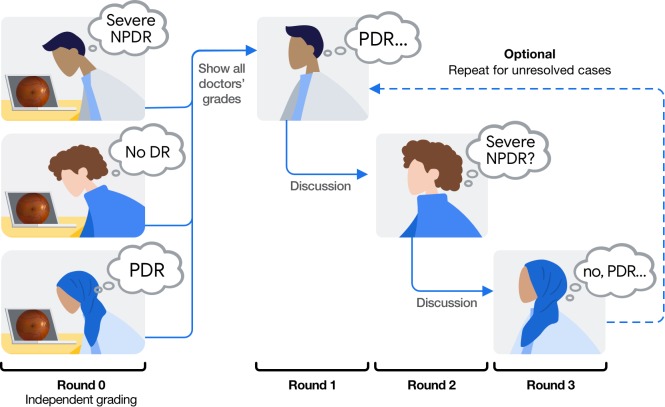
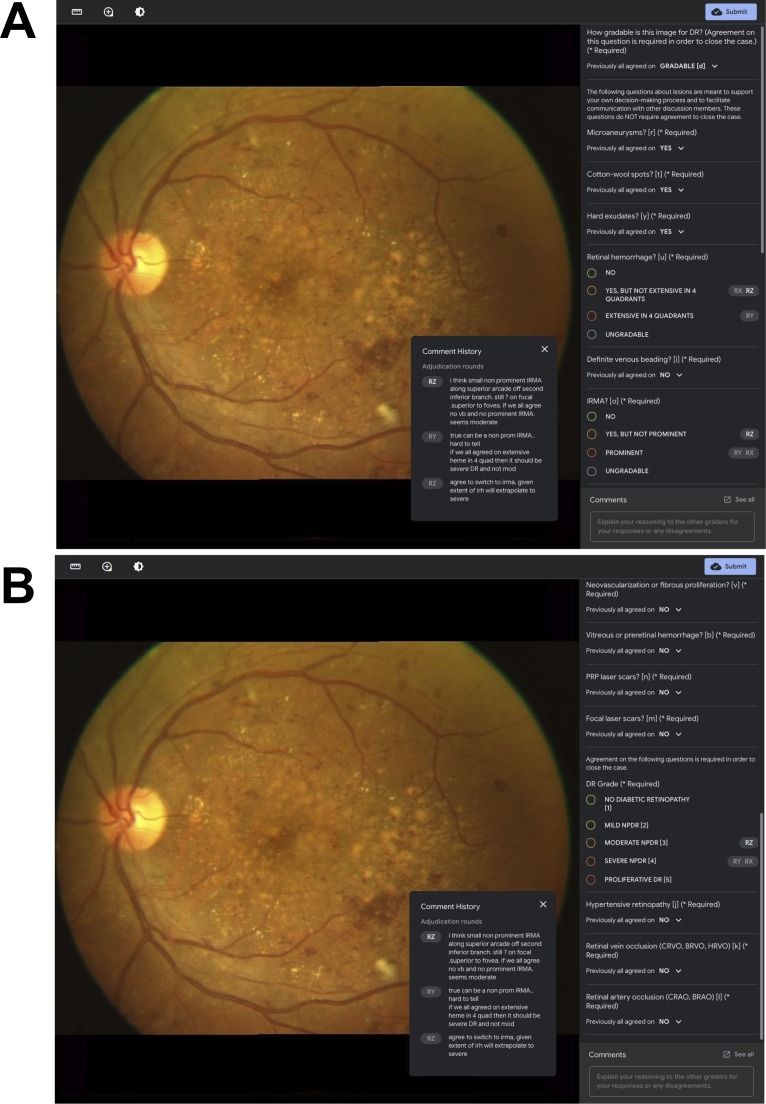
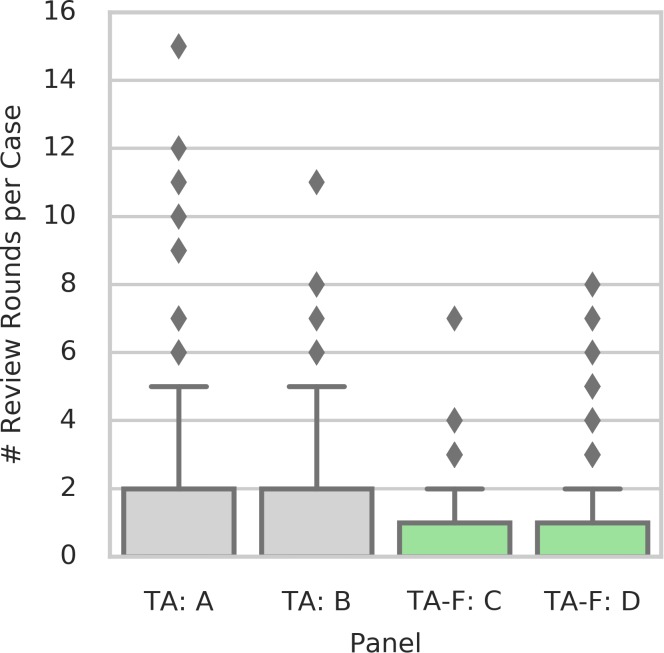
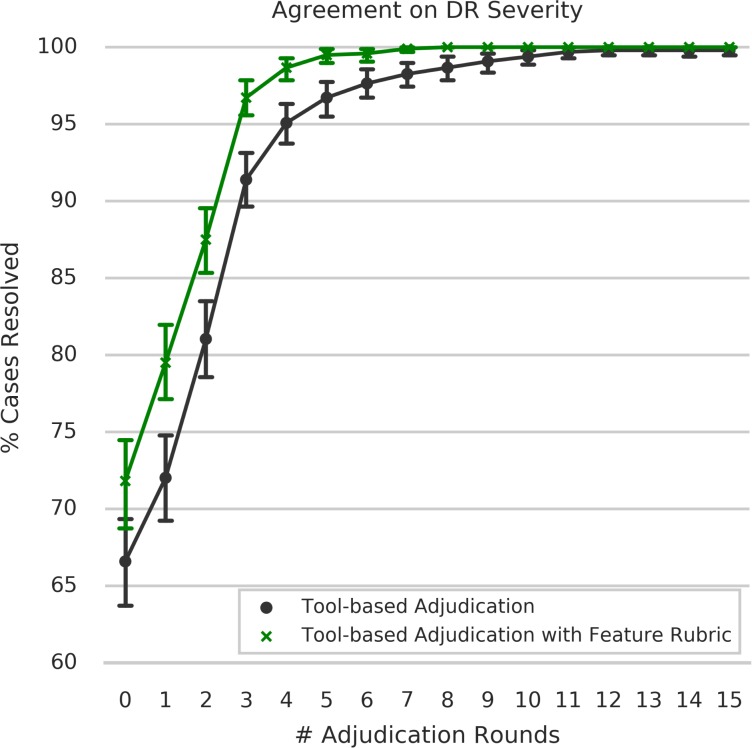
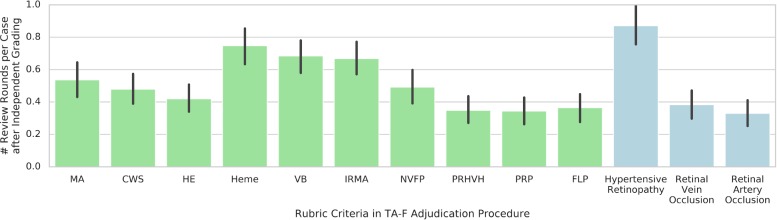
Methods: We compared three different procedures for adjudicating DR severity assessments among retina specialist panels, including (1) in-person adjudication based on a previously described procedure (Baseline), (2) remote, tool-based adjudication for assessing DR severity alone (TA), and (3) remote, tool-based adjudication using a feature-based rubric (TA-F). We developed a system allowing graders to review images remotely and asynchronously. For both TA and TA-F approaches, images with disagreement were reviewed by all graders in a round-robin fashion until disagreements were resolved. Five panels of three retina specialists each adjudicated a set of 499 retinal fundus images (1 panel using Baseline, 2 using TA, and 2 using TA-F adjudication). Reliability was measured as grade agreement among the panels using Cohen's quadratically weighted kappa. Efficiency was measured as the number of rounds needed to reach a consensus for tool-based adjudication.
Results: The grades from remote, tool-based adjudication showed high agreement with the Baseline procedure, with Cohen's kappa scores of 0.948 and 0.943 for the two TA panels, and 0.921 and 0.963 for the two TA-F panels. Cases adjudicated using TA-F were resolved in fewer rounds compared with TA (P < 0.001; standard permutation test).
Conclusions: Remote, tool-based adjudication presents a flexible and reliable alternative to in-person adjudication for DR diagnosis. Feature-based rubrics can help accelerate consensus for tool-based adjudication of DR without compromising label quality.
Translational relevance: This approach can generate reference standards to validate automated methods, and resolve ambiguous diagnoses by integrating into existing telemedical workflows.
Keywords: adjudication; diabetic retinopathy; retinal imaging; teleophthalmology.
Copyright 2019 The Authors.
Figures
References
-
- Ting DSW, Cheung GCM, Wong TY. Diabetic retinopathy: global prevalence, major risk factors, screening practices and public health challenges: a review. Clin Exp Ophthalmol. 2016;44:260–277. - PubMed
-
- International Council of Ophthalmology. International clinical diabetic retinopathy disease severity scale, detailed table. Available at: http://www.icoph.org/resources/45/International-Clinical-Diabetic-Retino.... Accessed January 6. 2019
-
- Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs–an extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology. 1991;98(5 Suppl):786–806. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
