

A clinical decision support tool may help to optimise vedolizumab therapy in Crohn's disease
- PMID: 31867766
- PMCID: PMC7028036
- DOI: 10.1111/apt.15609
A clinical decision support tool may help to optimise vedolizumab therapy in Crohn's disease
Erratum in
-
Corrigendum.Aliment Pharmacol Ther. 2021 Apr;53(8):963. doi: 10.1111/apt.16332. Aliment Pharmacol Ther. 2021. PMID: 33745181 Free PMC article. No abstract available.
Abstract
Background: A clinical decision support tool (CDST) has been validated for predicting treatment effectiveness of vedolizumab (VDZ) in Crohn's disease.
Aim: To assess the utility of this CDST for predicting exposure-efficacy and disease outcomes.
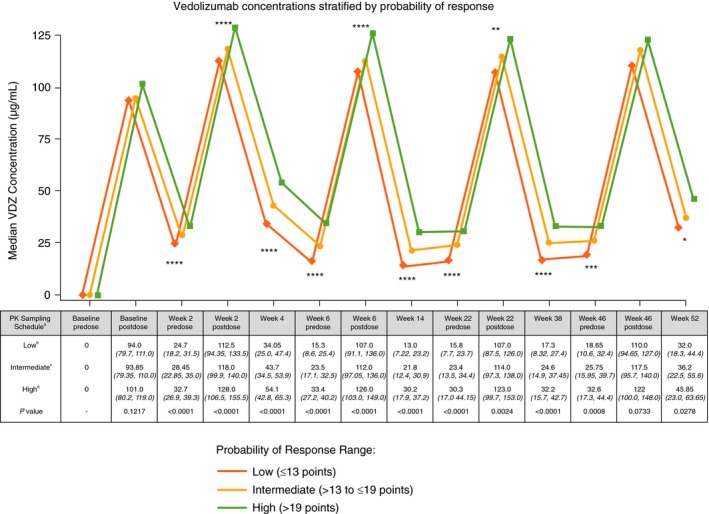
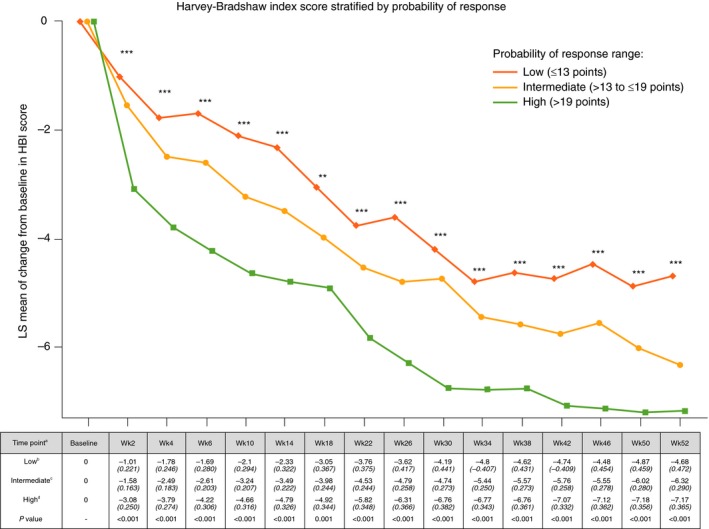
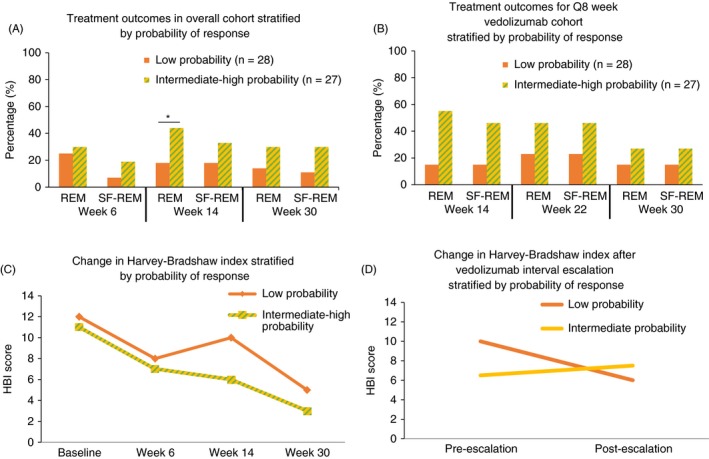
Methods: Using data from three independent datasets (GEMINI, GETAID and VICTORY), we assessed clinical remission rates and measured VDZ exposure, rapidity of onset of action, response to dose optimisation and progression to surgery by CDST-defined response groups (low, intermediate and high).
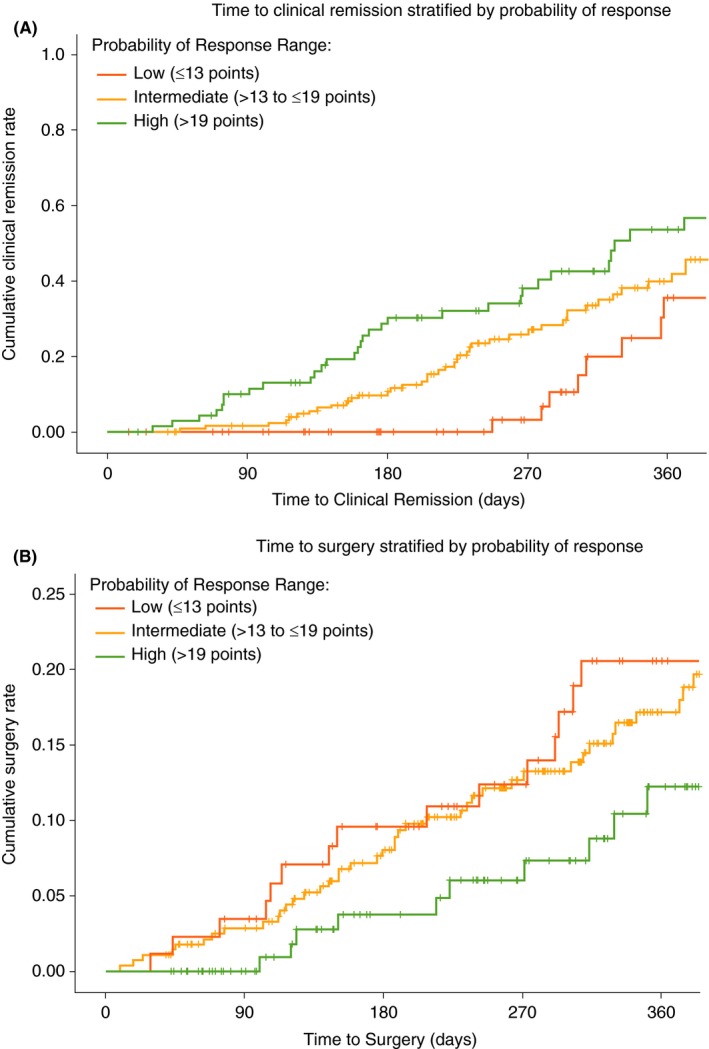
Results: A linear relationship existed between CDST-defined groups, measured VDZ exposure, rapidity of onset of action and efficacy in GEMINI through week 52 (P < 0.001 at all time points across three CDST-defined groups). In GETAID, CDST predicted differences in clinical remission at week 14 (AUC = 0.68) and rapidity of onset of action (P = 0.04) between probability groups. The high-probability patients did not benefit from shortening of infusion intervals, and differences in onset of action between the high-intermediate and low-probability groups within GETAID were no longer significant when including low-probability patients who received a week 10 infusion. CDST predicted a twofold increase in surgery risk over 12 months of VDZ therapy among low- to intermediate-probability vs high-probability patients (adjusted HR 2.06, 95% CI 1.33-3.21).
Conclusions: We further extended the clinical utility of a previously validated VDZ CDST, which accurately predicts at baseline exposure-efficacy relationships and rapidity of onset of action and could be used to help identify patients who would most benefit from interval shortening and those most likely to require surgery while on active therapy.
© 2019 The Authors. Alimentary Pharmacology & Therapeutics published by John Wiley & Sons Ltd.
Figures
Comment in
-
Editorial: a clinical decision tool to identify patients who might benefit most from intensified dosing in the biological era-getting nearer? Authors' reply.Aliment Pharmacol Ther. 2020 Apr;51(7):738-739. doi: 10.1111/apt.15671. Aliment Pharmacol Ther. 2020. PMID: 32162371 No abstract available.
-
Editorial: a clinical decision tool to identify patients who might benefit most from intensified dosing in the biological era-getting nearer?Aliment Pharmacol Ther. 2020 Apr;51(7):737-738. doi: 10.1111/apt.15634. Aliment Pharmacol Ther. 2020. PMID: 32162373 No abstract available.
-
Editorial: the road to elimination of viral hepatitis-another promising real-world experience.Aliment Pharmacol Ther. 2020 Jul;52(2):405-406. doi: 10.1111/apt.15837. Aliment Pharmacol Ther. 2020. PMID: 32592247 No abstract available.
References
-
- Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as induction and maintenance therapy for Crohn's disease. N Engl J Med. 2013;369:711–721. - PubMed
-
- Engel T, Ungar B, Yung DE, Ben‐Horin S, Eliakim R, Kopylov U. Vedolizumab in IBD‐lessons from real‐world experience: a systematic review and pooled analysis. J Crohns Colitis. 2018;12:245–257. - PubMed
-
- Dreesen E, Verstockt B, Bian S, et al. Evidence to support monitoring of vedolizumab trough concentrations in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2018;16:1937–1946. - PubMed
-
- Ungar B, Kopylov U, Yavzori M, et al. Association of vedolizumab level, anti‐drug antibodies, and alpha4beta7 occupancy with response in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2018;16:697–705.e7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical