

Contemporary utilization patterns and outcomes of thrombolytic administration for ischemic stroke among patients with cancer
- PMID: 31868139
- PMCID: PMC7924729
- DOI: 10.1177/1747493019895709
Contemporary utilization patterns and outcomes of thrombolytic administration for ischemic stroke among patients with cancer
Abstract
Background: Thrombolytic therapy significantly improves outcomes among patients with acute ischemic stroke. While cancer outcomes have dramatically improved, the utilization, safety, and mortality outcomes of patients with cancer who receive thrombolytic therapy for acute ischemic stroke are unknown.
Methods: Using a national database, we identified all hospitalizations for acute ischemic stroke requiring thrombolytic therapy between 2003 and 2015. Patients with contraindications to thrombolytic therapy were excluded. Following propensity score matching for comorbidity burden, trends in thrombolytic therapy use and its effect on in-hospital mortality, intracranial or all-cause bleeding, and the combined endpoint of mortality and all-cause bleeding, by presence/absence of cancer were evaluated. We also evaluated 30- and 90-day readmission rates post-thrombolytic therapy administration.
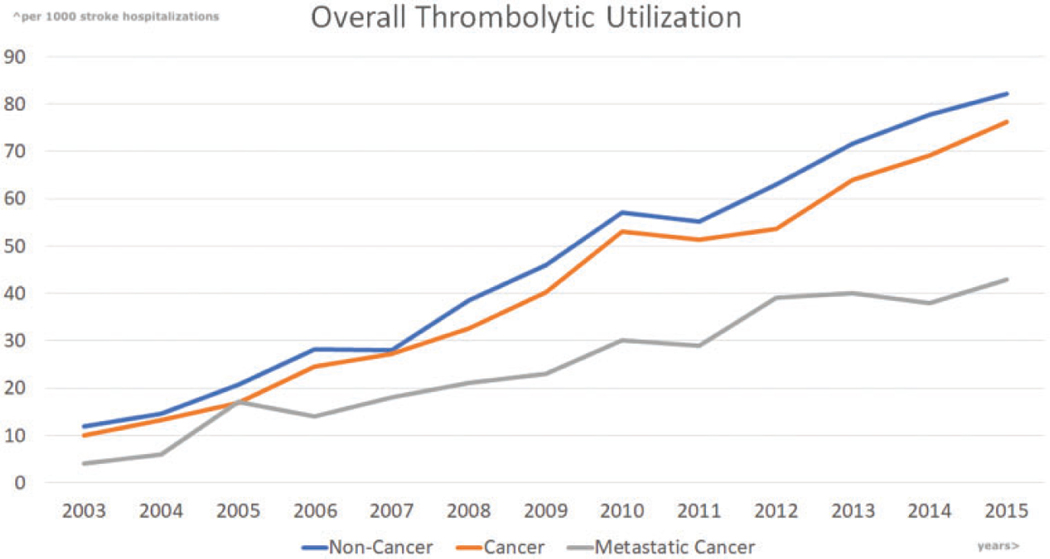
Results: We identified 237,687 acute ischemic stroke hospitalizations requiring thrombolytic therapy, of which 26,328 (11%) had an underlying cancer. Over the study period, thrombolytic therapy use increased across all acute ischemic stroke admissions, irrespective of cancer presence (12.4/1000 in 2003 to 81.1/1000 in 2015, P < 0.0001). However, thrombolytic therapy utilization differed by cancer presence (4.8% cancer vs.·5.1% non-cancer, P = 0.001). There was no difference in intracranial bleeding (9.6% vs. 9.7%), all-cause bleeding (13.2% vs. 13.2%), or in-hospital mortality (7.6% vs. 7.2%). While there was no difference in 30-day readmission rates by cancer presence (24% vs. 29%, P = 0.40), at 90-days, cancer patients saw higher readmission rates (17.2% vs. 13.3%, P = 0.02).
Conclusions: Contemporary thrombolytic therapy use for acute ischemic stroke has risen, irrespective of presence of cancer. Yet, patients with comorbid cancer appear to see lower rates of thrombolytic therapy use for acute ischemic stroke, despite no difference in the rate of intracranial bleeding or mortality after adjustment for comorbidities.
Keywords: Ischemic stroke; cancer; in-hospital outcomes; readmission; thrombolytic.
Conflict of interest statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation 2018; 137: e67–e492. - PubMed
-
- Siegel RL, Miller KD and Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68: 7–30. - PubMed
-
- Shapiro CL. Cancer survivorship. N Engl J Med 2018; 379: 2438–2450. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
