

Lead-I ECG for detecting atrial fibrillation in patients attending primary care with an irregular pulse using single-time point testing: A systematic review and economic evaluation
- PMID: 31869370
- PMCID: PMC6927656
- DOI: 10.1371/journal.pone.0226671
Lead-I ECG for detecting atrial fibrillation in patients attending primary care with an irregular pulse using single-time point testing: A systematic review and economic evaluation
Abstract
Background: Atrial fibrillation (AF) is the most common type of cardiac arrhythmia and is associated with increased risk of stroke and congestive heart failure. Lead-I electrocardiogram (ECG) devices are handheld instruments that can detect AF at a single-time point.
Purpose: To assess the diagnostic test accuracy, clinical impact and cost effectiveness of single-time point lead-I ECG devices compared with manual pulse palpation (MPP) followed by a 12-lead ECG for the detection of AF in symptomatic primary care patients with an irregular pulse.
Methods: Electronic databases (MEDLINE, MEDLINE Epub Ahead of Print and MEDLINE In-Process, EMBASE, PubMed and Cochrane Databases of Systematic Reviews, Cochrane Central Database of Controlled Trials, Database of Abstracts of Reviews of Effects, Health Technology Assessment Database) were searched to March 2018. Two reviewers screened the search results, extracted data and assessed study quality. Summary estimates of diagnostic accuracy were calculated using bivariate models. Cost-effectiveness was evaluated using an economic model consisting of a decision tree and two cohort Markov models.
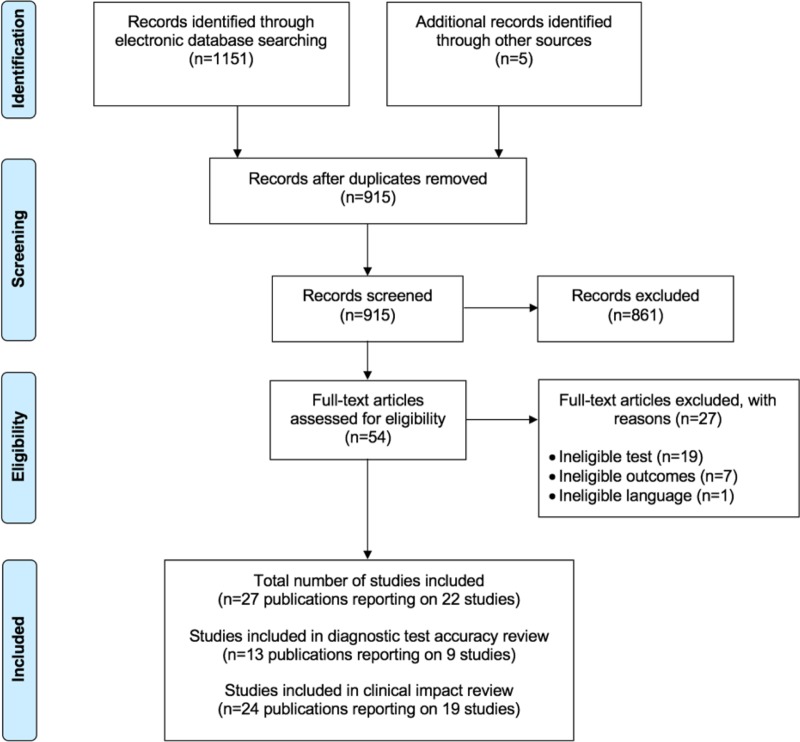
Results: Diagnostic accuracy The diagnostic accuracy (13 publications reporting on nine studies) and clinical impact (24 publications reporting on 19 studies) results are derived from an asymptomatic population (used as a proxy for people with signs or symptoms of AF). The summary sensitivity of lead-I ECG devices was 93.9% (95% confidence interval [CI]: 86.2% to 97.4%) and summary specificity was 96.5% (95% CI: 90.4% to 98.8%). Cost effectiveness The de novo economic model yielded incremental cost effectiveness ratios (ICERs) per quality adjusted life year (QALY) gained. The results of the pairwise analysis show that all lead-I ECG devices generate ICERs per QALY gained below the £20,000-£30,000 threshold. Kardia Mobile is the most cost effective option in a full incremental analysis. Lead-I ECG tests may identify more AF cases than the standard diagnostic pathway. This comes at a higher cost but with greater patient benefit in terms of mortality and quality of life.
Limitations: No published data evaluating the diagnostic accuracy, clinical impact or cost effectiveness of lead-I ECG devices for the target population are available.
Conclusions: The use of single-time point lead-I ECG devices in primary care for the detection of AF in people with signs or symptoms of AF and an irregular pulse appears to be a cost effective use of NHS resources compared with MPP followed by a 12-lead ECG, given the assumptions used in the base case model.
Registration: The protocol for this review is registered on PROSPERO as CRD42018090375.
Conflict of interest statement
Howard Thom reports personal fees from Novartis Pharma, Pfizer Inc, Hoffman La Roche, Bayer, and Janssen, all unrelated to the submitted work. James Mahon is Director of Coldingham Analytical Services. This commercial affiliation does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures

References
-
- National Institute for Health and Care Excellence (NICE). Clinical knowledge summaries: atrial fibrillation. 2015. Available from: https://cks.nice.org.uk/atrial-fibrillation#!topicsummary [accessed January 2018].
-
- Public Health England. Atrial fibrillation prevalence estimates in England: application of recent population estimates of AF in Sweden. 2017. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil... [accessed January 2018].
-
- Duarte R, Stainthorpe A, Greenhalgh J, Richardson M, Marshall T, Hall M, et al. The clinical and cost effectiveness of lead-I electrocardiogram (ECG) devices for detecting atrial fibrillation using single-time point testing in primary care—Protocol 2018. Available from: https://www.nice.org.uk/guidance/dg35/documents/final-protocol.
-
- National Institute for Health and Care Excellence (NICE). Atrial fibrillation: management. clinical guideline CG180. 2014. Available from: https://www.nice.org.uk/guidance/cg180/chapter/Introduction [accessed January 2018]. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
