

Considering adjuvant therapy for stage II melanoma
- PMID: 31869447
- PMCID: PMC7065103
- DOI: 10.1002/cncr.32585
Considering adjuvant therapy for stage II melanoma
Abstract
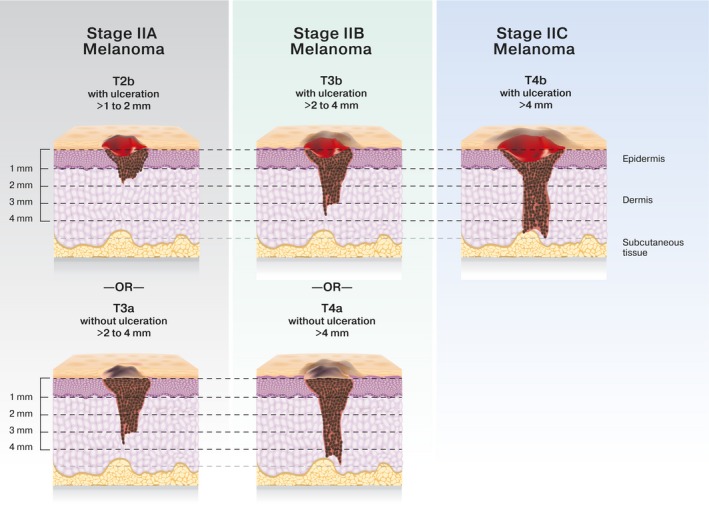
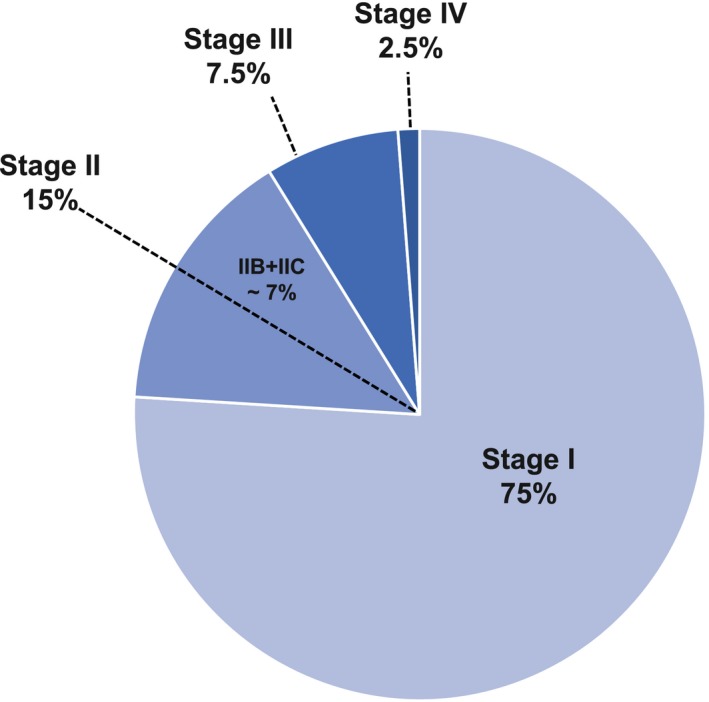
Melanoma is among the few cancers that demonstrate an increasing incidence over time. Simultaneously, this trend has been marked by an epidemiologic shift to earlier stage at diagnosis. Before 2011, treatment options were limited for patients with metastatic disease, and the median overall survival was less than 1 year. Since then, the field of melanoma therapeutics has undergone major changes. The use of anti-CTLA-4 and anti-PD1 immune checkpoint inhibitors and combination BRAF/MEK inhibitors for patients with BRAF V600 mutations has significantly extended survival and allowed some patients to remain in durable disease remission off therapy. It has now been confirmed that these classes of agents have a benefit for patients with stage III melanoma after surgical resection, and anti-PD1 and BRAF/MEK inhibitors are standards of care in this setting. Some patients with stage II disease (lymph node-negative; American Joint Committee on Cancer stage IIB and IIC) have worse melanoma-specific survival relative to some patients with stage III disease. Given these results, expanding the population of patients who are considered for adjuvant therapy to include those with stage II melanoma has become a priority, and randomized phase 3 clinical trials are underway. Moving into the future, the validation of patient risk-stratification and treatment-benefit prediction models will be important to improve the number needed to treat and limit exposure to toxicity in the large population of patients with early stage melanoma.
Keywords: BRAF; PD1; adjuvant therapy; immunotherapy; melanoma; pd-1; risk stratification; stage II; targeted therapy.
© 2019 The Authors. Cancer published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Conflict of interest statement
Andrew S. Poklepovic reports personal fees from Novartis, Merck, Bristol‐Myers Squibb, and Castle Biosciences outside the submitted work. Jason J. Luke reports research support from Array, CheckMate, Evelo, and Palleon, all outside the submitted work; institutional research support for clinical trials from AbbVie, Boston Biomedical, Bristol‐Myers Squibb, Celldex, Compugen, Corvus, EMD Serono, Delcath, Five Prime, FLX Bio, Genentech, Immunocore, Incyte, Leap, MedImmune, Macrogenics, Novartis, Pharmacyclics, Merck, Tesaro, and Xencor, all outside the submitted work; personal fees from 7 Hills, Actym, Alphamab Oncology, Mavu, Pyxis, Springbank, Tempest; personal fees from 7 Hills, AbbVie, Actym, Akrevia, Alphamab Oncology, Array, Astellas, AstraZeneca, Bayer, Bristol‐Myers Squibb, Compugen, EMD Serono, IDEAYA, Immunocore, Incyte, Janssen, Jounce, Leap, Mavu, Merck, Mersana, Novartis, Pyxis, RefleXion, Spring Bank, Tempest, and Vividion, all outside the submitted work; travel expenses from Akrevia, Array, AstraZeneca, Bayer, Bristol‐Myers Squibb, Castle, CheckMate, EMD Serono, IDEAYA, Immunocore, Incyte, Janssen, Jounce, Merck, Mersana, Novartis, RefleXion, all outside the submitted work; serves on the TTC Oncology Data and Safety Monitoring Board outside the submitted work; and holds provisional patent 15/612,657 (Cancer Immunotherapy) and provisional patent PCT/US18/36052 (Microbiome Biomarkers for Anti‐PD‐1/PD‐L1 Responsiveness: Diagnostic, Prognostic, and Therapeutic Uses Thereof).
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5‐29. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7‐30. - PubMed
-
- National Cancer Institute, Division of Cancer Control and Population Science . Research Emphasis. Division of Cancer Control and Population Sciences, National Cancer Institute, National Institutes of Health; 2018. Accessed November 11, 2018. http://cancercontrol.cancer.gov/research-emphasis/index.html
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
