Association between hydroxocobalamin administration and acute kidney injury after smoke inhalation: a multicenter retrospective study
- PMID: 31870461
- PMCID: PMC6929494
- DOI: 10.1186/s13054-019-2706-0
Association between hydroxocobalamin administration and acute kidney injury after smoke inhalation: a multicenter retrospective study
Abstract
Background: The use of hydroxocobalamin has long been advocated for treating suspected cyanide poisoning after smoke inhalation. Intravenous hydroxocobalamin has however been shown to cause oxalate nephropathy in a single-center study. The impact of hydroxocobalamin on the risk of acute kidney injury (AKI) and survival after smoke inhalation in a multicenter setting remains unexplored.
Methods: We conducted a multicenter retrospective study in 21 intensive care units (ICUs) in France. We included patients admitted to an ICU for smoke inhalation between January 2011 and December 2017. We excluded patients discharged at home alive within 24 h of admission. We assessed the risk of AKI (primary endpoint), severe AKI, major adverse kidney (MAKE) events, and survival (secondary endpoints) after administration of hydroxocobalamin using logistic regression models.
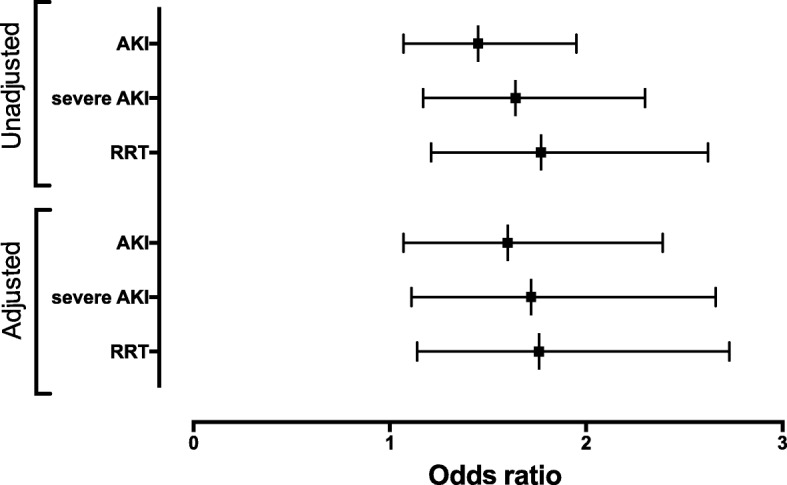
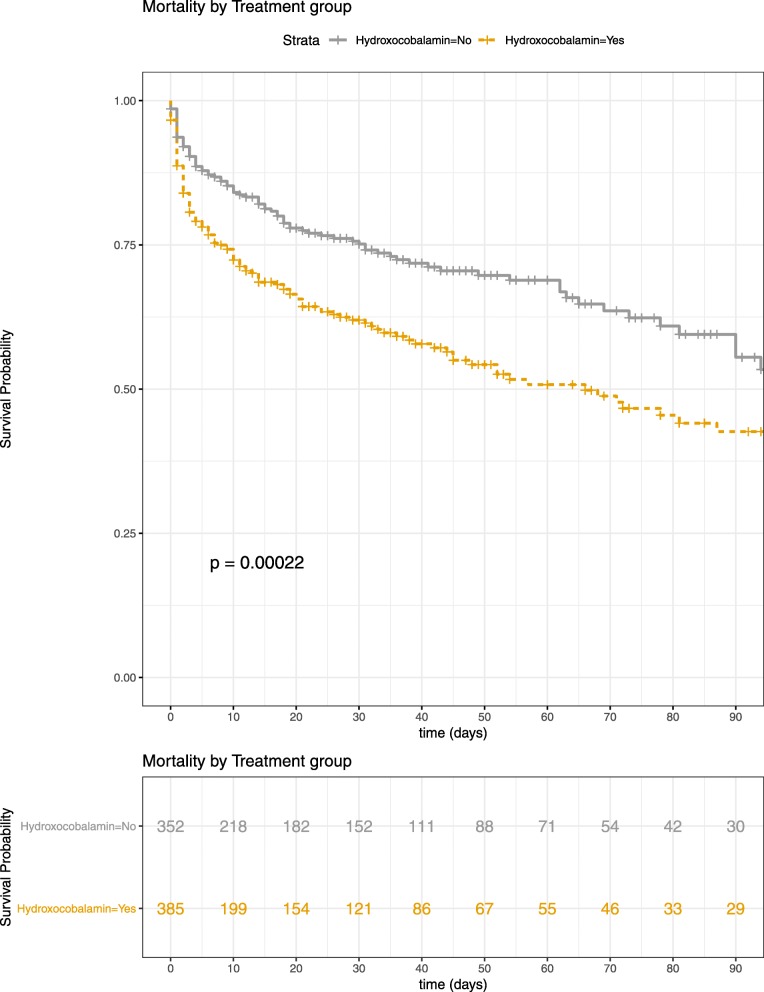
Results: Among 854 patients screened, 739 patients were included. Three hundred six and 386 (55.2%) patients received hydroxocobalamin. Mortality in ICU was 32.9% (n = 243). Two hundred eighty-eight (39%) patients developed AKI, including 186 (25.2%) who developed severe AKI during the first week. Patients who received hydroxocobalamin were more severe and had higher mortality (38.1% vs 27.2%, p = 0.0022). The adjusted odds ratio (95% confidence interval) of AKI after intravenous hydroxocobalamin was 1.597 (1.055, 2.419) and 1.772 (1.137, 2.762) for severe AKI; intravenous hydroxocobalamin was not associated with survival or MAKE with an adjusted odds ratio (95% confidence interval) of 1.114 (0.691, 1.797) and 0.784 (0.456, 1.349) respectively.
Conclusion: Hydroxocobalamin was associated with an increased risk of AKI and severe AKI but was not associated with survival after smoke inhalation.
Trial registration: ClinicalTrials.gov, NCT03558646.
Keywords: Acute kidney injury; Burn; Hydroxocobalamin; Intensive care unit; Mortality; Smoke inhalation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures