

Anti-PD-L1 (atezolizumab) as an immune primer and concurrently with extended-field chemoradiotherapy for node-positive locally advanced cervical cancer
- PMID: 31871115
- PMCID: PMC7310564
- DOI: 10.1136/ijgc-2019-001012
Anti-PD-L1 (atezolizumab) as an immune primer and concurrently with extended-field chemoradiotherapy for node-positive locally advanced cervical cancer
Erratum in
-
Correction: Anti-PD-L1 (atezolizumab) as an immune primer and concurrently with extended-field chemoradiotherapy for node-positive locally advanced cervical cancer.Int J Gynecol Cancer. 2020 Jul;30(7):1084. doi: 10.1136/ijgc-2019-001012corr1. Epub 2020 May 4. Int J Gynecol Cancer. 2020. PMID: 32371424 Free PMC article. No abstract available.
-
Correction: Anti-PD-L1 (atezolizumab) as an immune primer and concurrently with extended-field chemoradiotherapy for node-positive locally advanced cervical cancer.Int J Gynecol Cancer. 2020 Aug;30(8):1266. doi: 10.1136/ijgc-2019-001012corr2. Int J Gynecol Cancer. 2020. PMID: 32769164 Free PMC article. No abstract available.
Abstract
Background: There is a lack of data exploring the use and optimal timing of immunotherapy and chemoradiation therapy (CRT) in node-positive cervical cancer. Further translational research into mechanisms of response and resistance to immunotherapy in advanced cervical cancer is warranted.
Primary objectives: To determine if sequencing of atezolizumab and CRT result in differential immune activation, as determined by clonal expansion of T cell receptor beta (TCRB) repertoires in peripheral blood on day 21.
Study hypothesis: There is a difference for clonal expansion of T cell receptor beta repertoires in the peripheral blood at day 21 between the priming and concurrent atezolizumab and CRT in Arm A vs the concurrent atezolizumab and CRT in Arm B.
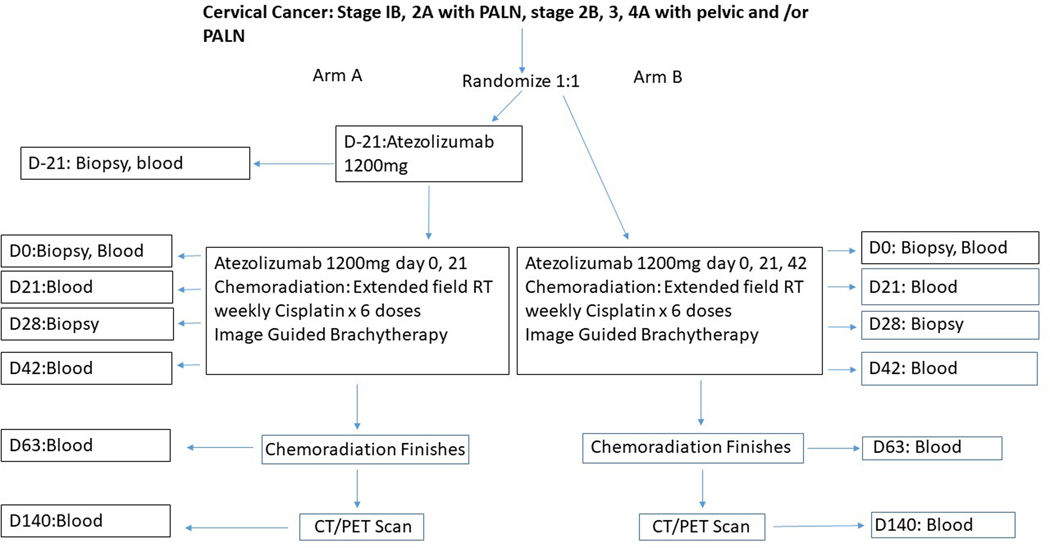
Trial design: Locally advanced cervical cancer patients with lymph node-positive disease will be randomized on this open-label, randomized trial with two experimental arms. Arm A will get one dose of atezolizumab prior to cisplatin CRT, and then two subsequent doses of atezolizumab during the CRT, and Arm B will get three doses during CRT. Patients will be followed for 2 years to assess outcomes.
Major inclusion/exclusion criteria: Patients must have histologically confirmed, newly diagnosed advanced cervical cancer (squamous cell carcinoma, adenocarcinoma, and adenosquamous cell carcinoma): FIGO 2009 clinical stages IB2/IIA with positive para-aortic nodes, or FIGO 2009 clinical stages IIB/IIIB/IVA with positive pelvic or para-aortic lymph nodes. Exclusion criteria include those who had a prior hysterectomy or lymph node dissection.
Primary endpoints: Clonal expansion of TCRB) repertoires in peripheral blood on day 21.
Sample size: The sample size will be 40 patients.
Estimated dates for completing accrual and presenting results: We estimate accrual to finish by the summer of 2020 with presentation of results to follow in 2021.
Trial registration: NCT03738228.
Keywords: Cervical Cancer; Gynecology; Radiation.
© IGCS and ESGO 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Macdonald OK, Chen J, Dodson M, et al.: Prognostic significance of histology and positive lymph node involvement following radical hysterectomy in carcinoma of the cervix. Am J Clin Oncol 32:411–6, 2009 - PubMed
-
- Dyer BA, Zamarin D, Eskandar RN, et al.: Role of Immunotherapy in the Management of Locally Advanced and Recurrent/Metastatic Cervical Cancer. J Natl Compr Canc Netw 17:91–97, 2019 - PubMed
-
- Munoz N, Bosch FX, de Sanjose S, et al.: Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med 348:518–27, 2003 - PubMed
-
- Cogliano V, Baan R, Straif K, et al.: Carcinogenicity of human papillomaviruses. Lancet Oncol 6:204, 2005 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
