

Traumatic spondyloptosis of L3 with incomplete neurological involvement: A case report
- PMID: 31872021
- PMCID: PMC6911902
- DOI: 10.1016/j.tcr.2019.100248
Traumatic spondyloptosis of L3 with incomplete neurological involvement: A case report
Abstract
High-energy traumas frequently result in lumbar spine fractures such as spondyloptosis is the maximum expression of instability and severity. The management of spondyloptosis is complex and, essentially, surgical. It usually presents with irreversible neurological compromise. This paper aimed to present a case of lumbar spondyloptosis and its early confrontation, partial neurological involvement, and progressive postoperative retrieval.
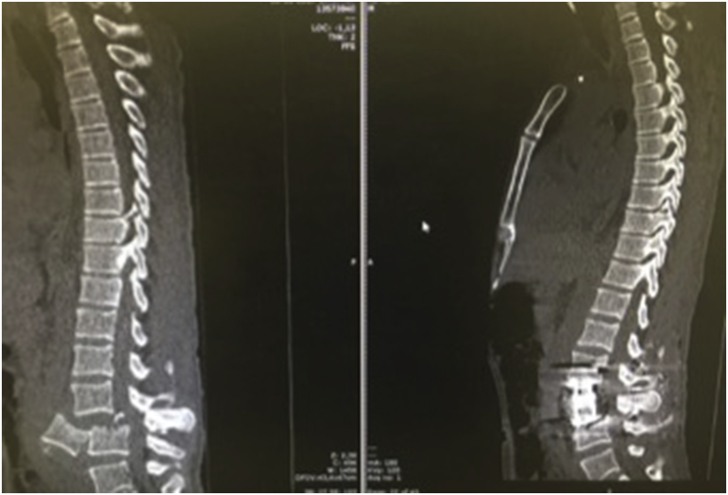
Clinical case: A male patient aged 42 years had multiple injuries with asymmetric paraparesis and sphincter involvement. Computed tomography (CT) revealed L3 vertebral spondyloptosis detached from the rest of the spine, spinal canal stenosis, sagittal imbalance, and angular kyphosis. Surgical resolution was defined by performing an en bloc corpectomy through lumbotomy and the installation of an expandable cage with posterior transpedicular fixation of L2-L4, thereby recovering the spinal canal diameter, lumbar lordosis, sagittal balance, and improving motor function progressively.
Conclusion: Complex spinal injuries warrant an early resolution by a trained surgical team to ensure normal spinal parameters and to achieve a progressive neurological recovery.
Keywords: Intraoperative neurophysiological monitoring; Lordosis; Lumbar vertebrae; Spinal fusion; Trauma.
© 2019 The Authors.
Figures



Similar articles
-
Traumatic lateral spondyloptosis of L2 with complete neurological deficit: A case report.Trauma Case Rep. 2020 Jul 29;29:100339. doi: 10.1016/j.tcr.2020.100339. eCollection 2020 Oct. Trauma Case Rep. 2020. PMID: 32817876 Free PMC article.
-
Mid-lumbar traumatic spondyloptosis without neurological deficit: A case report and literature review.Medicine (Baltimore). 2020 Mar;99(12):e19578. doi: 10.1097/MD.0000000000019578. Medicine (Baltimore). 2020. PMID: 32195971 Free PMC article. Review.
-
Congenital lumbar spinal stenosis: a prospective, control-matched, cohort radiographic analysis.Spine J. 2005 Nov-Dec;5(6):615-22. doi: 10.1016/j.spinee.2005.05.385. Spine J. 2005. PMID: 16291100 Clinical Trial.
-
Treatment strategy on traumatic mid-lumbar spondyloptosis with concomitant multiple injuries: A case report and literature review.Chin J Traumatol. 2023 Jan;26(1):33-40. doi: 10.1016/j.cjtee.2022.06.006. Epub 2022 Jun 28. Chin J Traumatol. 2023. PMID: 35868949 Free PMC article. Review.
-
Traumatic spondyloptosis of the lumbar spine: closed reduction and internal fixation.Spine (Phila Pa 1976). 2013 Dec 1;38(25):E1636-40. doi: 10.1097/BRS.0b013e3182a64412. Spine (Phila Pa 1976). 2013. PMID: 23921328
Cited by
-
Unstable Thoracolumbar Injuries: Factors Affecting the Decision for Short-Segment vs Long-Segment Posterior Fixation.Int J Spine Surg. 2022 Aug;16(5):772-778. doi: 10.14444/8337. Epub 2022 Aug 17. Int J Spine Surg. 2022. PMID: 35977752 Free PMC article.
-
Traumatic lateral spondyloptosis of L2 with complete neurological deficit: A case report.Trauma Case Rep. 2020 Jul 29;29:100339. doi: 10.1016/j.tcr.2020.100339. eCollection 2020 Oct. Trauma Case Rep. 2020. PMID: 32817876 Free PMC article.
-
Irreducible L5/S1 Spondyloptosis in Over 20 Years After Neglected Trauma Treated with Modified Grob's Technique - Case Report.Int Med Case Rep J. 2023 Sep 12;16:537-543. doi: 10.2147/IMCRJ.S428840. eCollection 2023. Int Med Case Rep J. 2023. PMID: 37720364 Free PMC article.
-
Traumatic thoracolumbar spondyloptosis of T12-L1 with stable hemodynamics: A case report.Int J Surg Case Rep. 2024 Jul;120:109703. doi: 10.1016/j.ijscr.2024.109703. Epub 2024 Apr 24. Int J Surg Case Rep. 2024. PMID: 38851070 Free PMC article.
-
Acute Traumatic Lumbar Spondyloptosis with Complete Neurological Deficit: A Case Report and Literature Review.J Orthop Case Rep. 2025 Apr;15(4):180-185. doi: 10.13107/jocr.2025.v15.i04.5492. J Orthop Case Rep. 2025. PMID: 40212502 Free PMC article.
References
-
- Gitelman A., Most M.J., Stephen M. Traumatic thoracic spondyloptosis without neurologic deficit and in situ treatment with fusion. Am J Orthop (Belle Mead NJ) 2009;38:E162–E165. - PubMed
-
- Mishra A., Agrawal D., Gupta D., Sinha S., Satyarthee G., Singh P. Traumatic spondyloptosis: a series of 20 patients. J. Neurosurg. Spine. 2015;22(6):647–652. - PubMed
-
- Garg M., Kumar A., Sawarkar D., Singh P., Agarwal D., Kale S. Traumatic lateral spondyloptosis: case series. World Neurosurg. 2018;113:E166–E171. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
