

Distinct interferon signatures and cytokine patterns define additional systemic autoinflammatory diseases
- PMID: 31874111
- PMCID: PMC7108905
- DOI: 10.1172/JCI129301
Distinct interferon signatures and cytokine patterns define additional systemic autoinflammatory diseases
Abstract
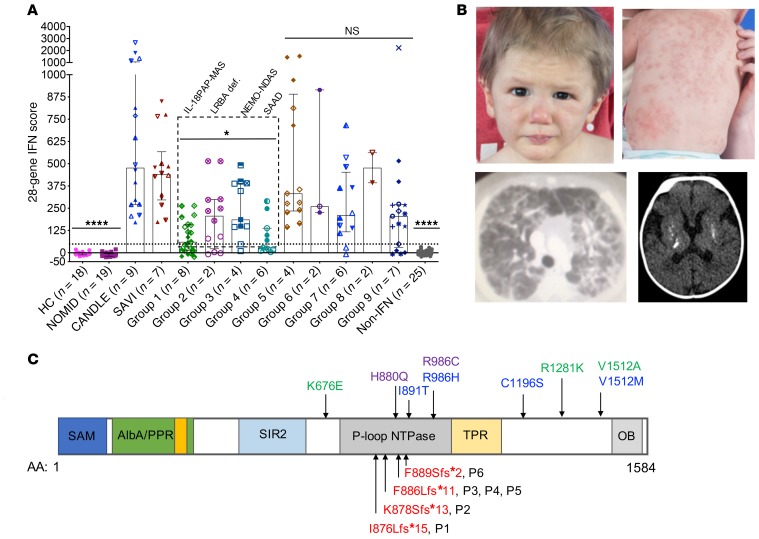
BACKGROUNDUndifferentiated systemic autoinflammatory diseases (USAIDs) present diagnostic and therapeutic challenges. Chronic interferon (IFN) signaling and cytokine dysregulation may identify diseases with available targeted treatments.METHODSSixty-six consecutively referred USAID patients underwent underwent screening for the presence of an interferon signature using a standardized type-I IFN-response-gene score (IRG-S), cytokine profiling, and genetic evaluation by next-generation sequencing.RESULTSThirty-six USAID patients (55%) had elevated IRG-S. Neutrophilic panniculitis (40% vs. 0%), basal ganglia calcifications (46% vs. 0%), interstitial lung disease (47% vs. 5%), and myositis (60% vs. 10%) were more prevalent in patients with elevated IRG-S. Moderate IRG-S elevation and highly elevated serum IL-18 distinguished 8 patients with pulmonary alveolar proteinosis (PAP) and recurrent macrophage activation syndrome (MAS). Among patients with panniculitis and progressive cytopenias, 2 patients were compound heterozygous for potentially novel LRBA mutations, 4 patients harbored potentially novel splice variants in IKBKG (which encodes NF-κB essential modulator [NEMO]), and 6 patients had de novo frameshift mutations in SAMD9L. Of additional 12 patients with elevated IRG-S and CANDLE-, SAVI- or Aicardi-Goutières syndrome-like (AGS-like) phenotypes, 5 patients carried mutations in either SAMHD1, TREX1, PSMB8, or PSMG2. Two patients had anti-MDA5 autoantibody-positive juvenile dermatomyositis, and 7 could not be classified. Patients with LRBA, IKBKG, and SAMD9L mutations showed a pattern of IRG elevation that suggests prominent NF-κB activation different from the canonical interferonopathies CANDLE, SAVI, and AGS.CONCLUSIONSIn patients with elevated IRG-S, we identified characteristic clinical features and 3 additional autoinflammatory diseases: IL-18-mediated PAP and recurrent MAS (IL-18PAP-MAS), NEMO deleted exon 5-autoinflammatory syndrome (NEMO-NDAS), and SAMD9L-associated autoinflammatory disease (SAMD9L-SAAD). The IRG-S expands the diagnostic armamentarium in evaluating USAIDs and points to different pathways regulating IRG expression.TRIAL REGISTRATIONClinicalTrials.gov NCT02974595.FUNDINGThe Intramural Research Program of the NIH, NIAID, NIAMS, and the Clinical Center.
Keywords: Genetic diseases; Immunology; Inflammation; Innate immunity; Monogenic diseases.
Conflict of interest statement
Figures




References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
