

Treatment of Anterior Cruciate Ligament Injuries in Professional Soccer Players by Orthopedic Surgeons
- PMID: 31875070
- PMCID: PMC6923647
- DOI: 10.1055/s-0039-1697017
Treatment of Anterior Cruciate Ligament Injuries in Professional Soccer Players by Orthopedic Surgeons
Abstract
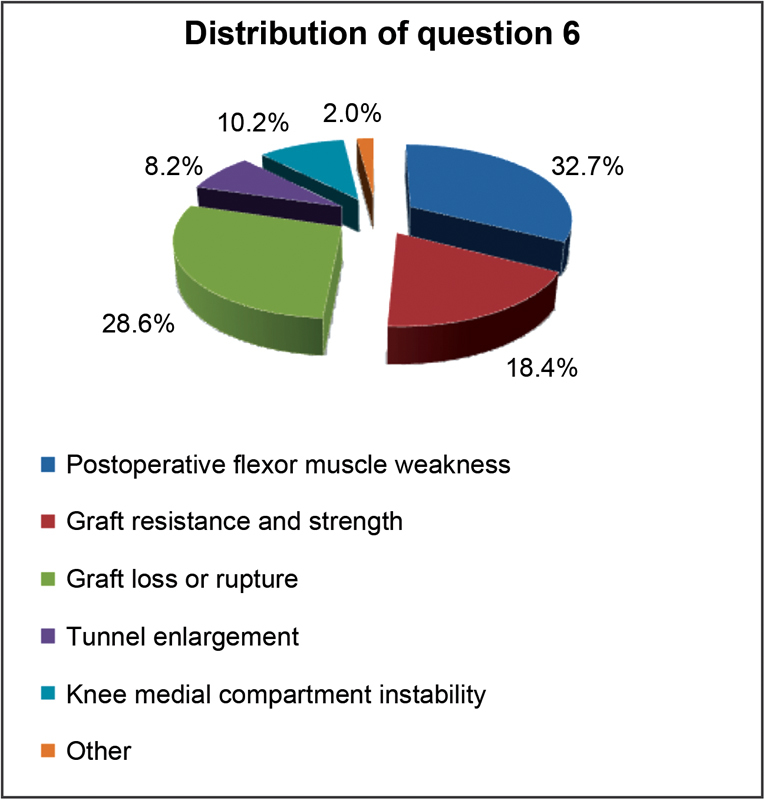
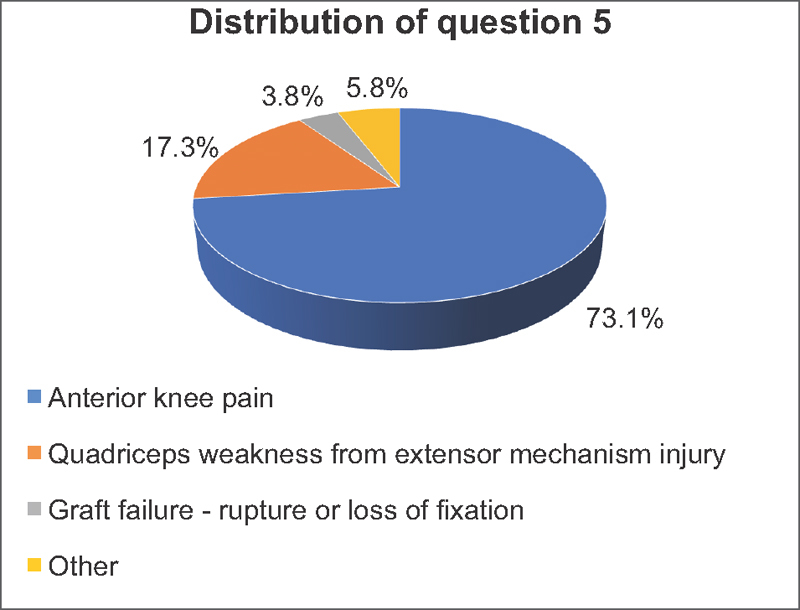
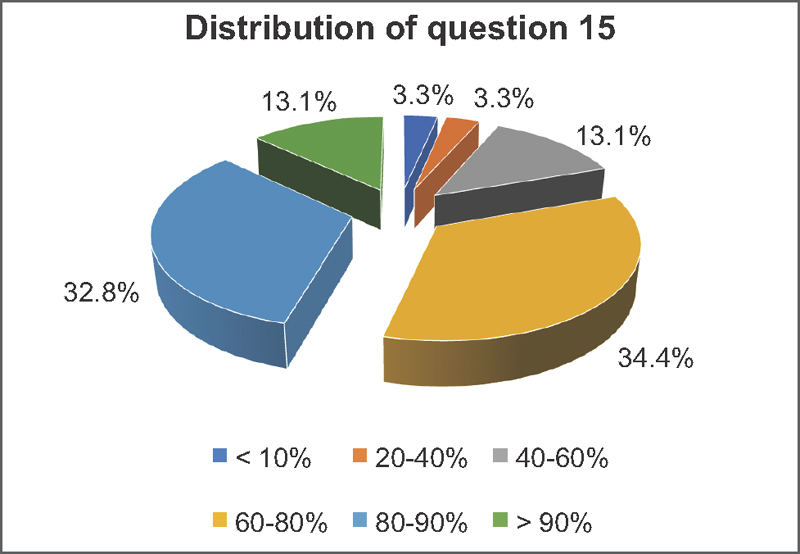
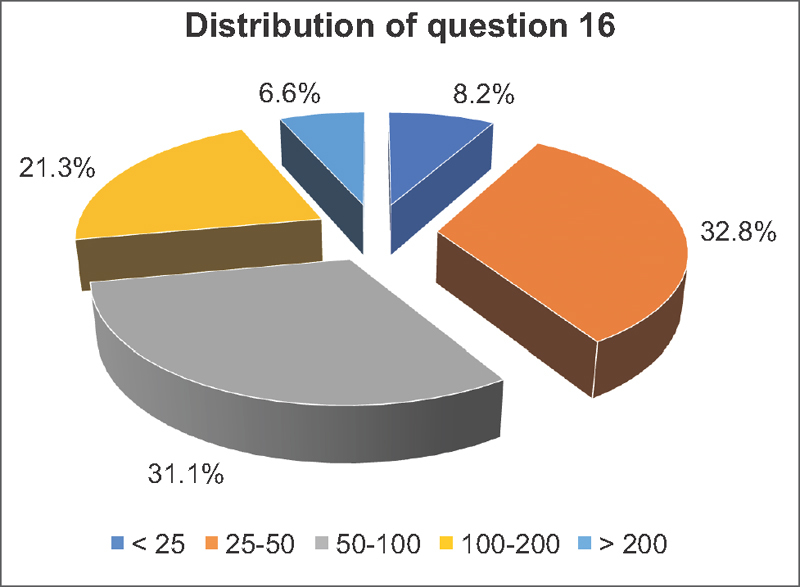
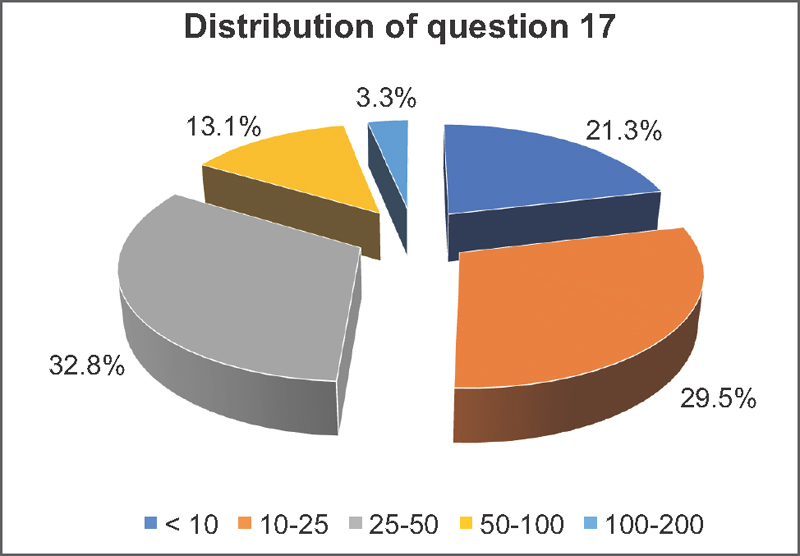
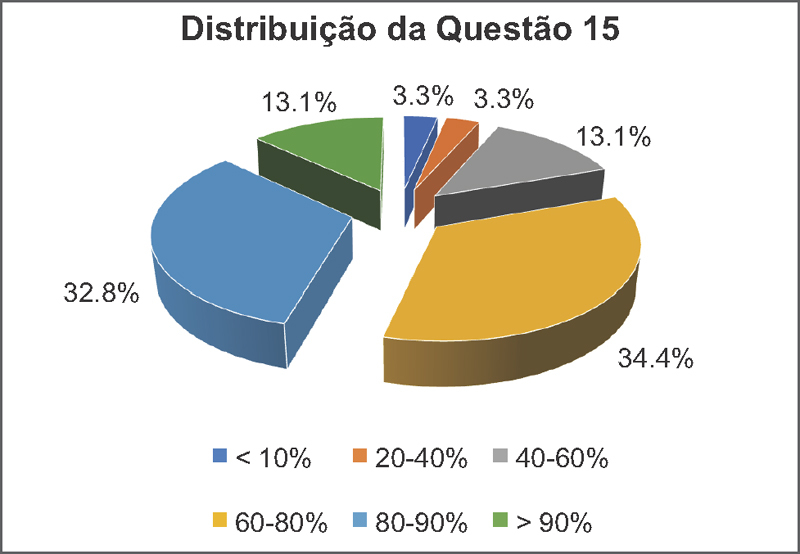
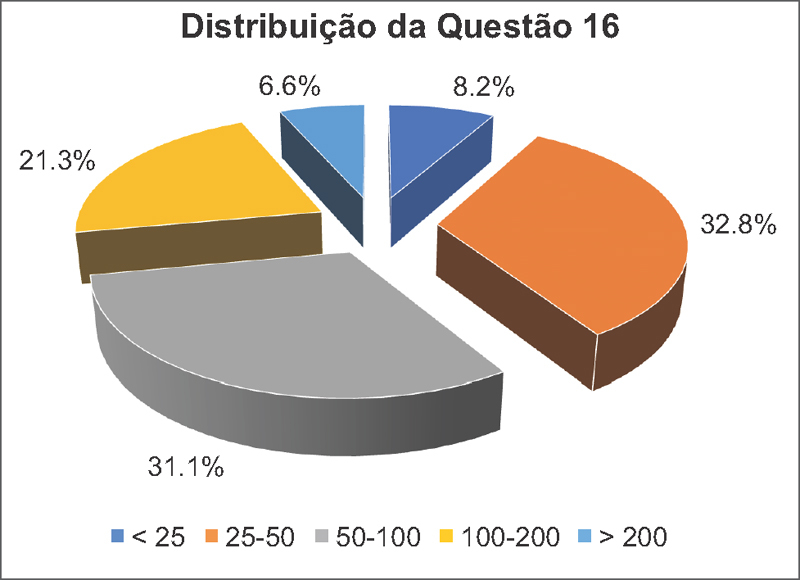
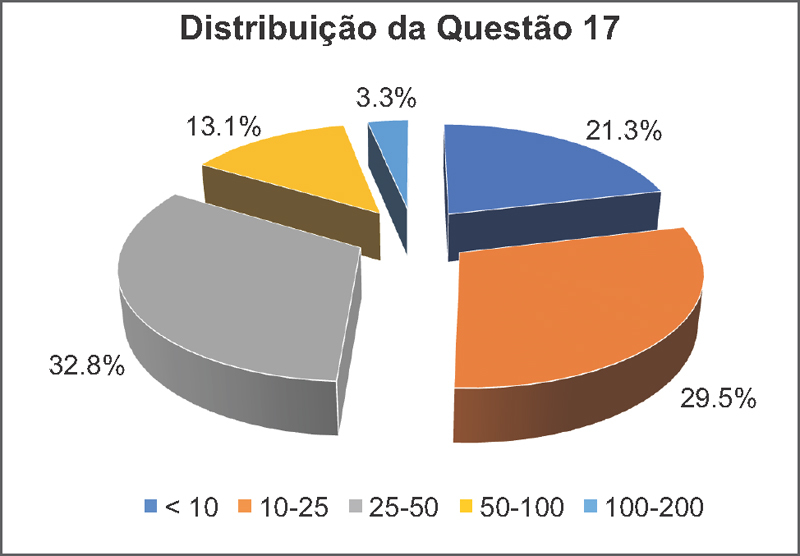
Objective To describe the treatment provided by specialists for ACL lesions in professional soccer players. Methods A cross-sectional study in which orthopedic surgeons affiliated to soccer teams competing in the Brazilian Soccer Championship answered a questionnaire about the treatment of ACL injuries in professional soccer players. Results The specialists wait between one to four weeks after the ACL injury to perform the surgical treatment. They use a single incision and single-bundle reconstruction, assisted by arthroscopy, femoral tunnel drilling by an accessory medial portal, and quadruple flexor tendon autografts or patellar tendon autografts. After three to four months, the players are allowed to run in a straight line; after four to six months, they begin to practice exercises with the ball without contact with other athletes; and, after six to eight months, they return to play. The main parameter used to determine the return to play is the isokinetic strength test. The specialists estimate that more than 90% of elite soccer players return to playing professionally after an ACL reconstruction, and 60 to 90% return to play at their prior or at a greater level of performance. Conclusion The present article successfully describes the main surgical practices and post-surgery management adopted by specialists in this highly-specific population of patients.
Keywords: anterior cruciate ligament; knee/surgery; rehabilitation; soccer.
Conflict of interest statement
Conflitos de Interesse Os autores declaram não haver conflitos de interesse.
Figures
References
-
- Fédération Internationale de Football Association. FIFA Big Count 2006. Disponível em:http://www.fifa.com/mm/document/fifafacts/bcoffsurv/bigcount.statspackag...
-
- Inklaar H. Soccer injuries. I: Incidence and severity. Sports Med. 1994;18(01):55–73. - PubMed
-
- Brito J, Soares J, Rebelo A N. Prevenção de lesões do ligamento cruzado anterior em futebolistas. Rev Bras Med Esporte. 2009;15(08):62–69.
LinkOut - more resources
Full Text Sources