

Treatment responses to Azithromycin and Ciprofloxacin in uncomplicated Salmonella Typhi infection: A comparison of Clinical and Microbiological Data from a Controlled Human Infection Model
- PMID: 31877141
- PMCID: PMC6948818
- DOI: 10.1371/journal.pntd.0007955
Treatment responses to Azithromycin and Ciprofloxacin in uncomplicated Salmonella Typhi infection: A comparison of Clinical and Microbiological Data from a Controlled Human Infection Model
Abstract
Background: The treatment of enteric fever is complicated by the emergence of antimicrobial resistant Salmonella Typhi. Azithromycin is commonly used for first-line treatment of uncomplicated enteric fever, but the response to treatment may be sub-optimal in some patient groups when compared with fluoroquinolones.
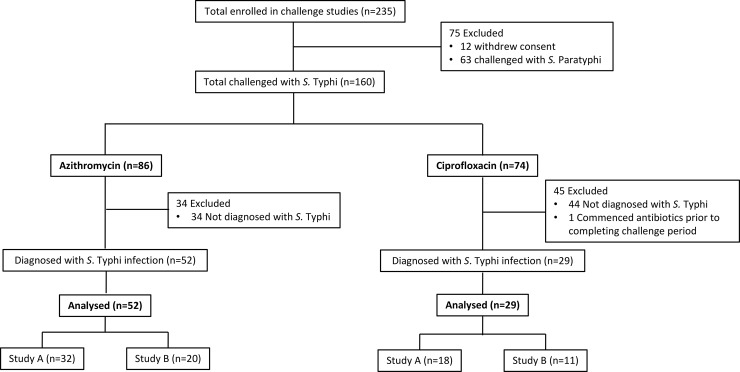
Methods: We performed an analysis of responses to treatment with azithromycin (500mg once-daily, 14 days) or ciprofloxacin (500mg twice-daily, 14 days) in healthy UK volunteers (18-60 years) enrolled into two Salmonella controlled human infection studies. Study A was a single-centre, open-label, randomised trial. Participants were randomised 1:1 to receive open-label oral ciprofloxacin or azithromycin, stratified by vaccine group (Vi-polysaccharide, Vi-conjugate or control Men-ACWY vaccine). Study B was an observational challenge/re-challenge study, where participants were randomised to challenge with Salmonella Typhi or Salmonella Paratyphi A. Outcome measures included fever clearance time, blood-culture clearance time and a composite measure of prolonged treatment response (persistent fever ≥38.0°C for ≥72 hours, persistently positive S. Typhi blood cultures for ≥72 hours, or change in antibiotic treatment). Both trials are registered with ClinicalTrials.gov (NCT02324751 and NCT02192008).
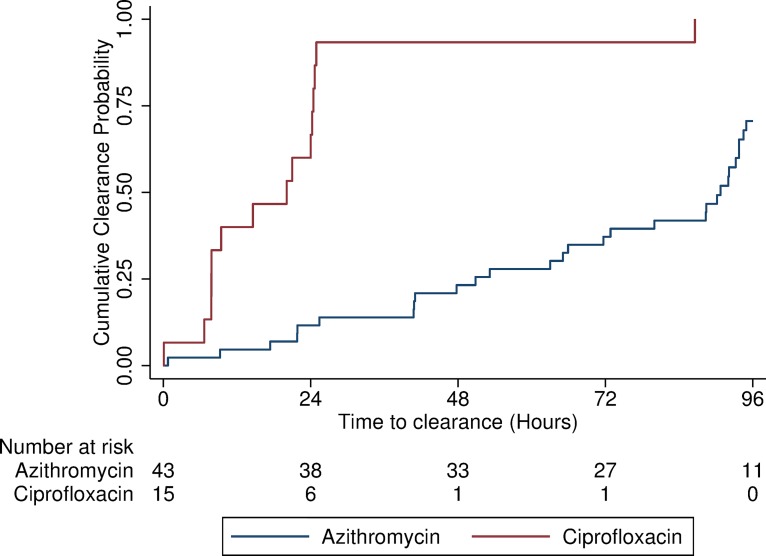
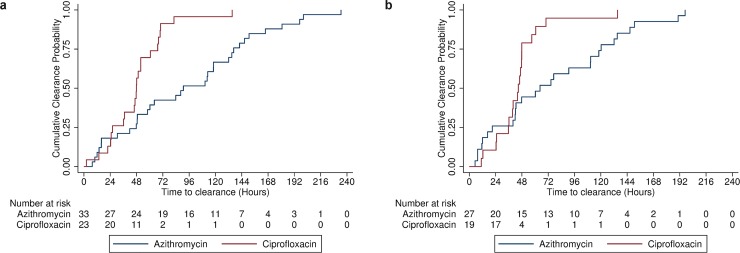
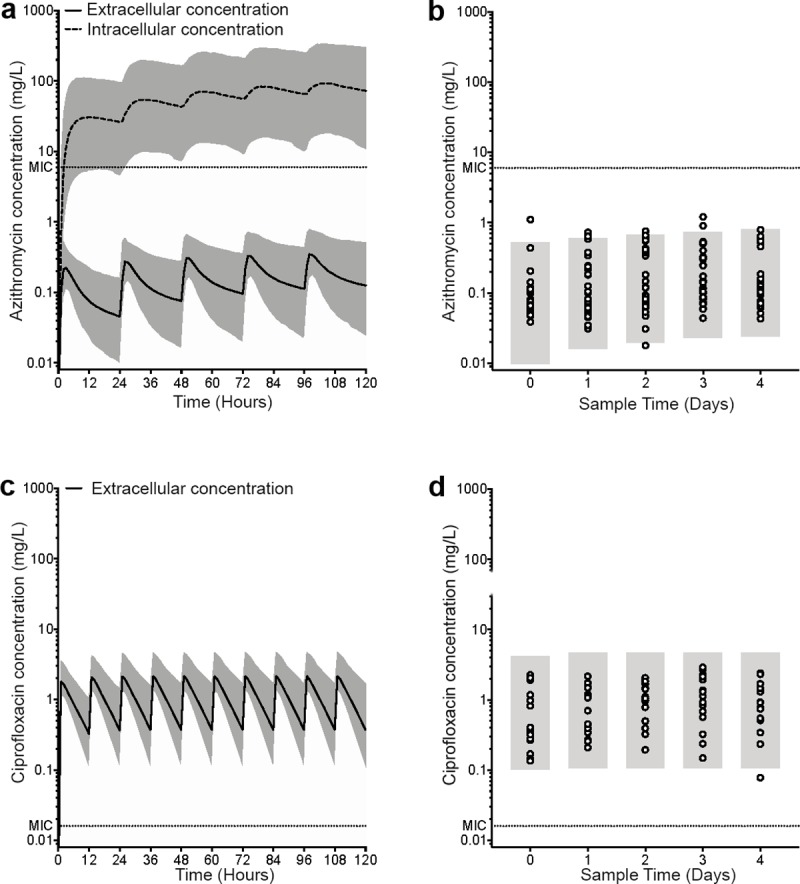
Findings: In 81 participants diagnosed with S. Typhi in two studies, treatment with azithromycin was associated with prolonged bacteraemia (median 90.8 hours [95% CI: 65.9-93.8] vs. 20.1 hours [95% CI: 7.8-24.3], p<0.001) and prolonged fever clearance times <37.5°C (hazard ratio 2.4 [95%CI: 1.2-5.0]; p = 0.02). Results were consistent when studies were analysed independently and in a sub-group of participants with no history of vaccination or previous challenge. A prolonged treatment response was observed significantly more frequently in the azithromycin group (28/52 [54.9%]) compared with the ciprofloxacin group (1/29 [3.5%]; p<0.001). In participants treated with azithromycin, observed systemic plasma concentrations of azithromycin did not exceed the minimum inhibitory concentration (MIC), whilst predicted intracellular concentrations did exceed the MIC. In participants treated with ciprofloxacin, the observed systemic plasma concentrations and predicted intracellular concentrations of ciprofloxacin exceeded the MIC.
Interpretation: Azithromycin at a dose of 500mg daily is an effective treatment for fully sensitive strains of S. Typhi but is associated with delayed treatment response and prolonged bacteraemia when compared with ciprofloxacin within the context of a human challenge model. Whilst the cellular accumulation of azithromycin is predicted to be sufficient to treat intracellular S. Typhi, systemic exposure may be sub-optimal for the elimination of extracellular circulating S. Typhi. In an era of increasing antimicrobial resistance, further studies are required to define appropriate azithromycin dosing regimens for enteric fever and to assess novel treatment strategies, including combination therapies.
Trial registration: ClinicalTrials.gov (NCT02324751 and NCT02192008).
Conflict of interest statement
AJP chairs the UK Department of Health’s (DH) Joint Committee on Vaccination and Immunisation (JCVI) and the European Medicines Agency Scientific Advisory Group on Vaccines, and is a member of the World Health Organization’s (WHO) Strategic Advisory Group of Experts. The views expressed in this manuscript are those of the authors and do not necessarily reflect the views of the JCVI, the DH, or the WHO. All other authors declare no conflicts of interest.
Figures
References
-
- Gay FP. Typhoid fever considered as a problem of scientific medicine [Internet]. 1918. Available: http://www.archive.org/details/cu31924000230502
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- MC_U137884181/MRC_/Medical Research Council/United Kingdom
- MC_PC_15002/MRC_/Medical Research Council/United Kingdom
- G1002586/MRC_/Medical Research Council/United Kingdom
- MC_UU_00008/1/MRC_/Medical Research Council/United Kingdom
- DH_/Department of Health/United Kingdom
- G1000800/MRC_/Medical Research Council/United Kingdom
- 17722/CRUK_/Cancer Research UK/United Kingdom
- MC_UU_12010/1/MRC_/Medical Research Council/United Kingdom
- MR/K021222/1/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- G0501975/MRC_/Medical Research Council/United Kingdom
- MC_PC_14111/MRC_/Medical Research Council/United Kingdom
- MC_PC_16052 /MRC_/Medical Research Council/United Kingdom
- 11331/CRUK_/Cancer Research UK/United Kingdom
- MR/N028376/1/MRC_/Medical Research Council/United Kingdom
- MR/K01577X/1/MRC_/Medical Research Council/United Kingdom
- G0800158/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
