

Comparison of 6-week PMTCT outcomes for HIV-exposed and HIV-unexposed infants in the era of lifelong ART: Results from an observational prospective cohort study
- PMID: 31877153
- PMCID: PMC6932788
- DOI: 10.1371/journal.pone.0226339
Comparison of 6-week PMTCT outcomes for HIV-exposed and HIV-unexposed infants in the era of lifelong ART: Results from an observational prospective cohort study
Abstract
Background: Lifelong antiretroviral therapy (ART) reduces mother-to-child HIV transmission (MTCT) and improves maternal health. Data on the outcomes of HIV-exposed infants (HEI) compared to their unexposed counterparts in the era of universal ART is limited. We compared birth and 6-week outcomes among infants born to HIV-positive and HIV-negative women in Lesotho.
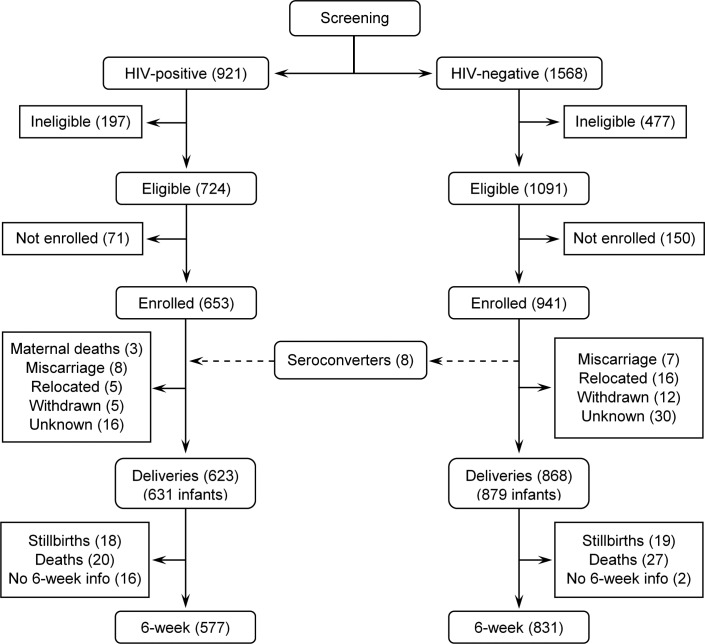
Methods: 941 HIV-negative and 653 HIV-positive pregnant women were enrolled in an observational cohort to evaluate the effectiveness of prevention of mother-to-child HIV transmission (PMTCT) program after implementation of universal maternal ART in 14 health facilities. Pregnancy, delivery, birth, and 6-week data were collected through participant interviews and medical record review. DNA PCR testing for HEI was conducted within 2 weeks of birth and at around 6 weeks of age. Data were analysed to estimate the distribution of birth outcomes, mortality, HIV transmission and HIV-free survival at 6 weeks.
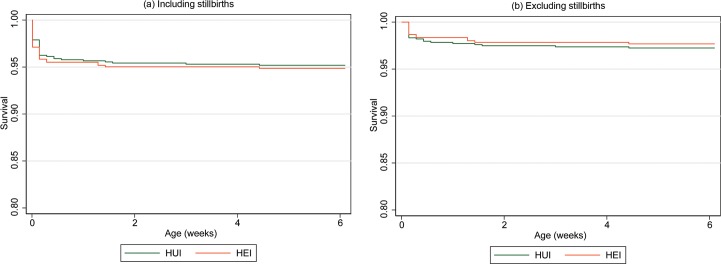
Results: HIV-positive women were older (mean age of 28.7 vs. 24.4 years) and presented for antenatal care earlier (mean gestational age of 23.0 weeks vs 25.3 weeks) than HIV-negative women. Prematurity was more frequent among HEI, 7.8% vs. 3.6%. There was no difference in rates of congenital anomalies between HEI (1.0%) and HIV-unexposed infants (HUI) (0.6%). Cumulative HIV transmission was 0.9% (N = 4/431) (95% CI:0.25-2.36) at birth and 1.0% (N = 6/583) (95% CI:0.38-2.23) at 6 weeks. Overall mortality, including stillbirths, was 5.2% and 6.0% by 6 weeks for HUI and HEI respectively. Among liveborn infants, 6-week HIV-free survival for HEI was 95.6% (95% CI:93.7-97.1) compared to 96.8% (95% CI:95.4-97.9) survival for HUI.
Conclusions: Implementation of universal maternal ART lowers MTCT at 6 weeks of age with no differences in congenital anomalies or early mortality between HIV exposed Infants and HIV unexposed infants. However, HIV exposed infants continue to have high rates of prematurity despite improved maternal health on ART.
Conflict of interest statement
The authors have declared that no competing interests exist
Figures
References
-
- The Kingdom Of Lesotho, Government of Lesotho. Final Report for a Joint Review of HIV/Tuberculosis and Hepatitis Programmes. 2 December, 2017. Available from: http://www.unaids.org/sites/default/files/country/documents/LSO_2018_cou.... Cited 2 January 2019.
-
- Kesho Bora Study Group. Triple antiretroviral compared with zidovudine and single-dose nevirapine prophylaxis during pregnancy and breastfeeding for prevention of mother-to-child transmission of HIV-1 (Kesho Bora study): a randomised controlled trial. Lancet Infect Dis. 2011;11(3): 171–80. 10.1016/S1473-3099(10)70288-7 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
