

Impact of MRI, CT, and Clinical Characteristics on Microbial Pathogen Detection Using CT-Guided Biopsy for Suspected Spondylodiscitis
- PMID: 31877797
- PMCID: PMC7019669
- DOI: 10.3390/jcm9010032
Impact of MRI, CT, and Clinical Characteristics on Microbial Pathogen Detection Using CT-Guided Biopsy for Suspected Spondylodiscitis
Abstract
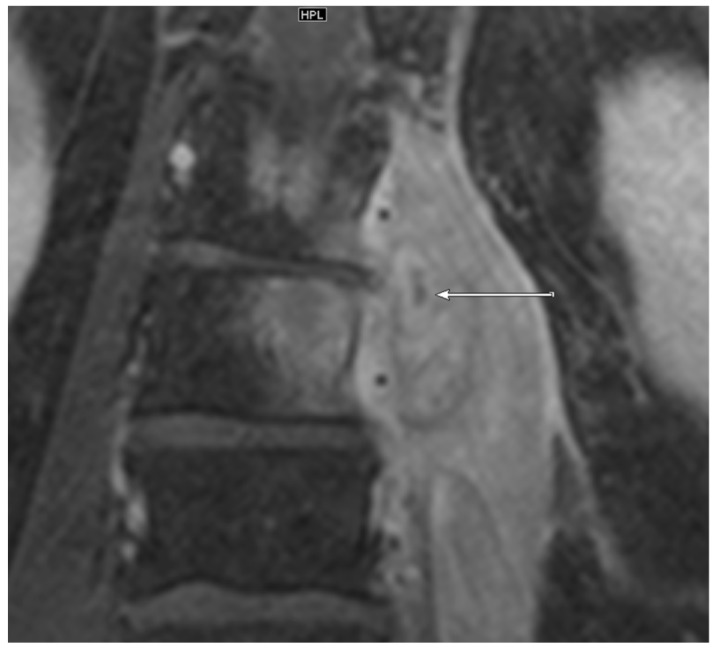
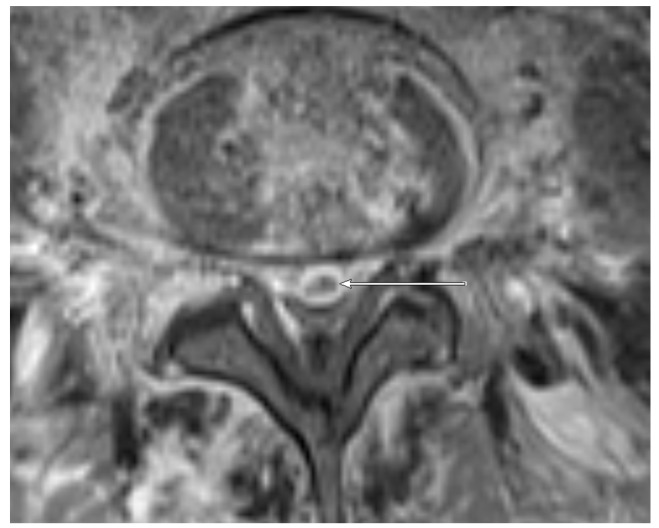
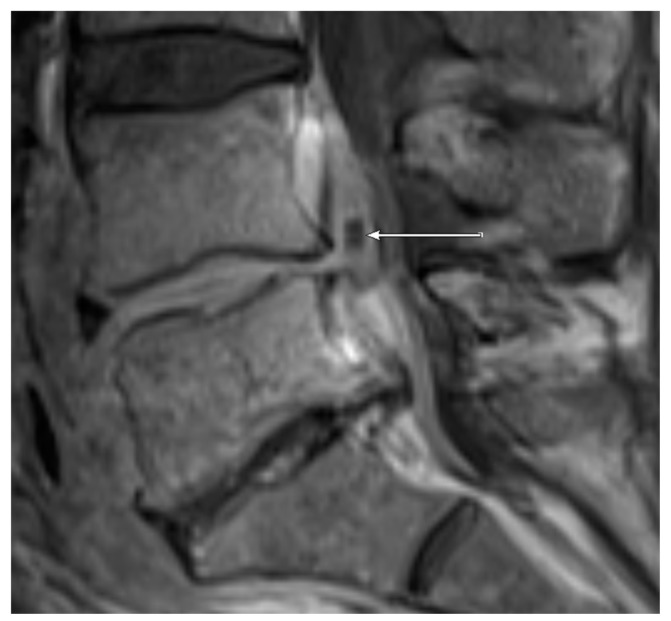
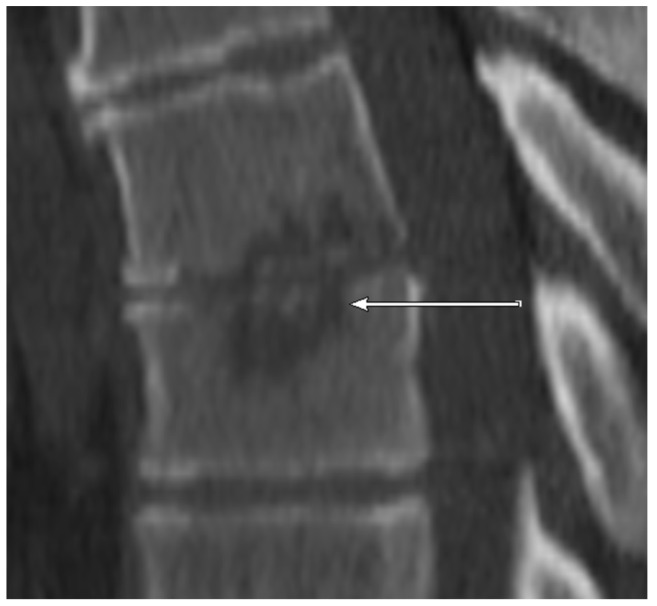
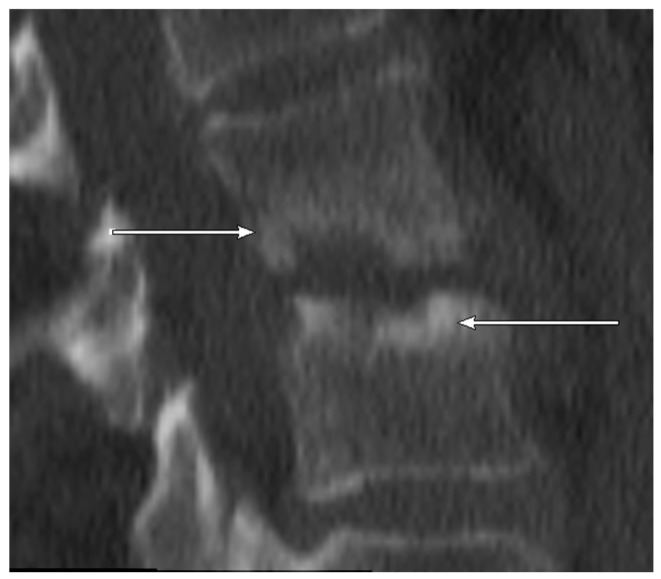
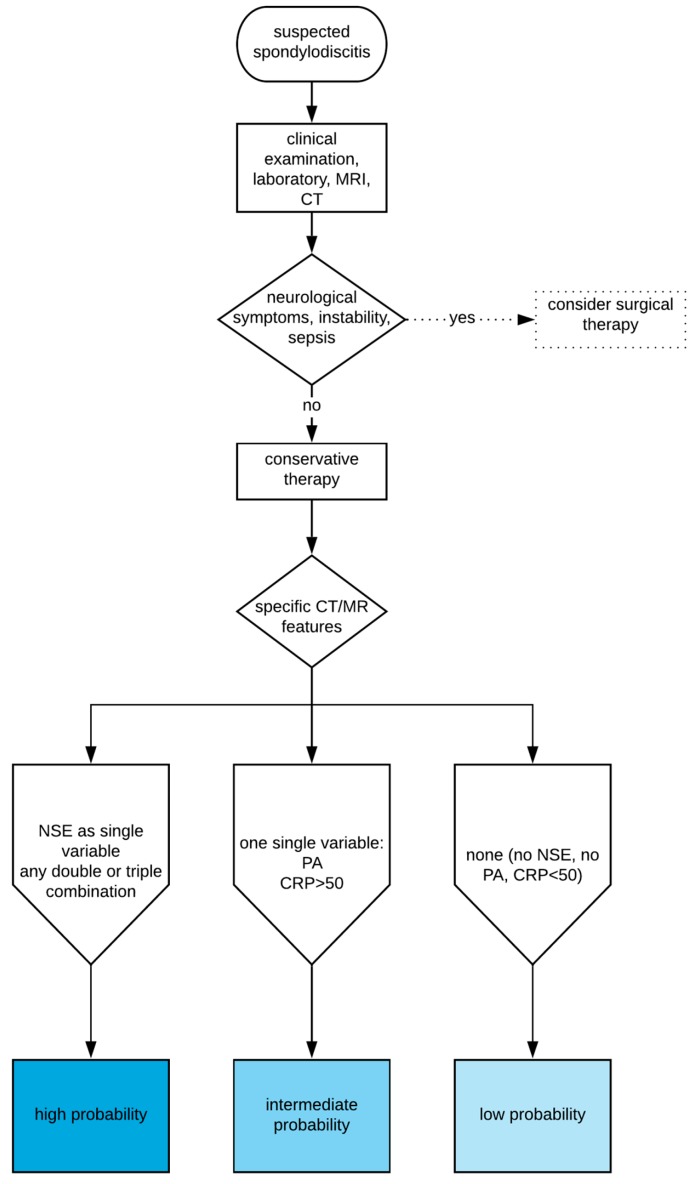
Spondylodiscitis accounts for 2-7% of osteomyelitis cases and is characterized by pain, systemic inflammation, and permanent neurological deficits. We aimed to identify imaging characteristics and clinical parameters to successfully predict microbiological pathogens by computed tomography (CT)-guided biopsy in suspected spondylodiscitis cases. Forty consecutive patients (mean age 65.1 years) with suspected spondylodiscitis underwent CT-guided biopsy. CT features (non-sclerotic endplate erosions (NSEs)), magnetic resonance criteria (paravertebral/epidural abscess (PA/EA) formation), and clinical data (C-reactive protein (CRP) > 50 mg/L) were assessed for their predictive potential. NSEs were detected in 6/11 (54.5%) and 1/29(3.4%) patients with positive and negative microbiology, respectively. PA and EA, respectively, were present in 7/11(63.6%) and 3/11 patients with positive microbiology and 7/29 (24.1%) and 2/29 patients with negative microbiology. CRP > 50 was observed in 7/11 (63.6%) and in 7/29 (24.1%) patients with positive and negative microbiology, respectively. Three double combinations possessed near-perfect specificity (PA + NSE, 100%; PA + CRP > 50, 96.6%; NSE + CRP > 50, 96.6%). The top three Youden indices included combinations with NSE. Since CT/magnetic resonance (MR) imaging and CRP are routinely used to evaluate spondylodiscitis, the presented diagnostic criteria and combinations can aid decision-making for biopsy.
Keywords: CRP; CT; MRI; biopsy; microbiology; spondylodiscitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
