

Synchronous and metachronous liver metastases in patients with colorectal cancer-towards a clinically relevant definition
- PMID: 31878952
- PMCID: PMC6933908
- DOI: 10.1186/s12957-019-1771-9
Synchronous and metachronous liver metastases in patients with colorectal cancer-towards a clinically relevant definition
Abstract
Background: Approximately 25% of patients with colorectal cancer (CRC) will have liver metastases classified as synchronous or metachronous. There is no consensus on the defining time point for synchronous/metachronous, and the prognostic implications thereof remain unclear. The aim of the study was to assess the prognostic value of differential detection at various defining time points in a population-based patient cohort and conduct a literature review of the topic.
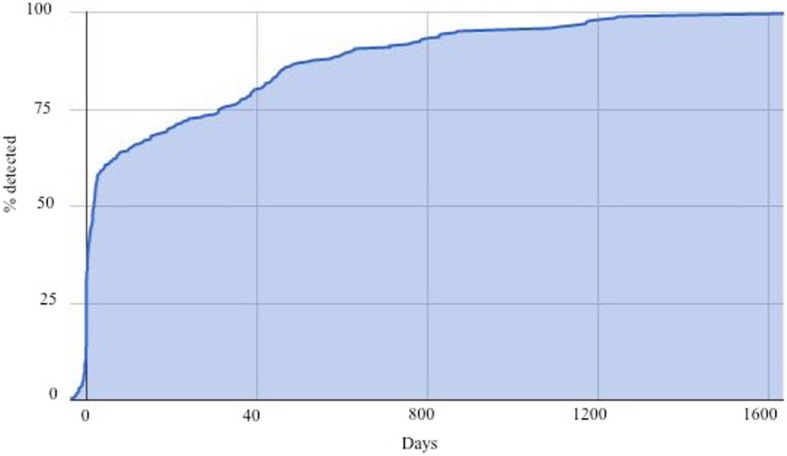
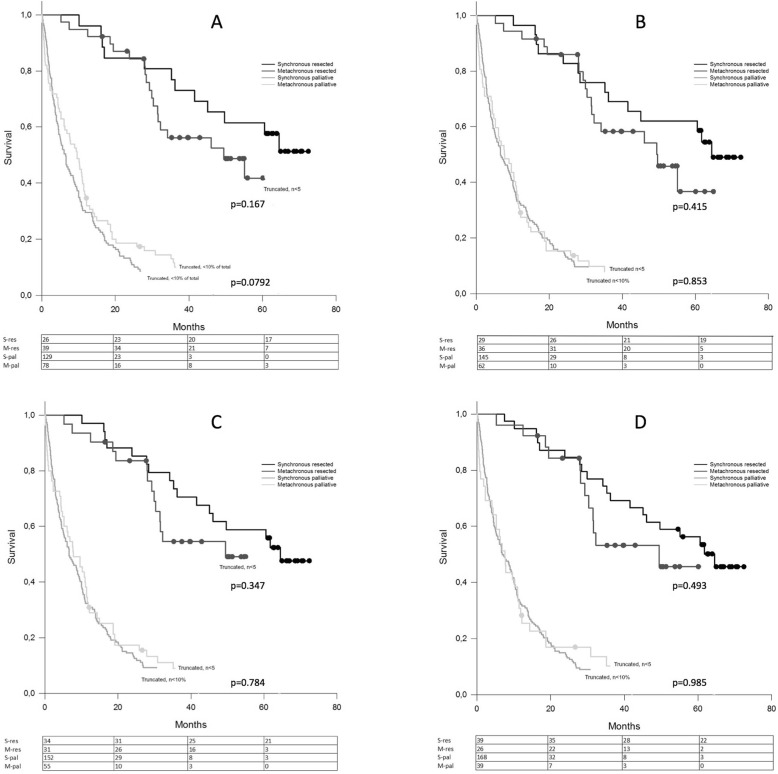
Methods: All patients diagnosed with CRC in the counties of Stockholm and Gotland, Sweden, during 2008 were included in the study and followed for 5 years or until death to identify patients diagnosed with liver metastases. Patients with liver metastases were followed from time of diagnosis of liver metastases for at least 5 years or until death. Different time points defining synchronous/metachronous detection, as reported in the literature and identified in a literature search of databases (PubMed, Embase, Cochrane library), were applied to the cohort, and overall survival was calculated using Kaplan-Meier curves and compared with log-rank test. The influence of synchronously or metachronously detected liver metastases on disease-free and overall survival as reported in articles forthcoming from the literature search was also assessed.
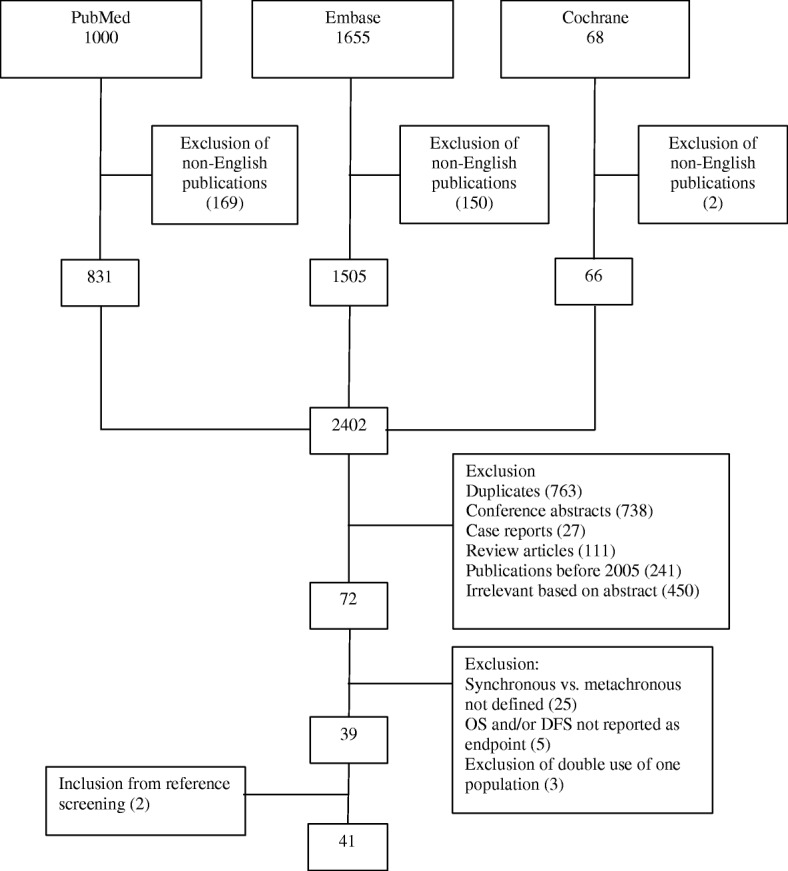
Results: Liver metastases were diagnosed in 272/1026 patients with CRC (26.5%). No statistically significant difference in overall survival for synchronous vs. metachronous detection at any of the defining time points (CRC diagnosis/surgery and 3, 6 and 12 months post-diagnosis/surgery) was demonstrated for operated or non-operated patients. In the literature search, 41 publications met the inclusion criteria. No clear pattern emerged regarding the prognostic significance of synchronous vs. metachronous detection.
Conclusion: Synchronous vs. metachronous detection of CRC liver metastases lacks prognostic value. Using primary tumour diagnosis/operation as standardized cut-off point to define synchronous/metachronous detection is semantically correct. In synchronous detection, it defines a clinically relevant group of patients where individualized multimodality treatment protocols will apply.
Keywords: Colorectal cancer; Liver metastases; Metachronous; Synchronous.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- de Jong MC, Pulitano C, Ribero D, Strub J, Mentha G, Schulick RD, et al. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: an international multi-institutional analysis of 1669 patients. Ann Surg. 2009;250(3):440–448. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
