

Pharmacotherapy for Pediatric Convulsive Status Epilepticus
- PMID: 31879852
- PMCID: PMC6982635
- DOI: 10.1007/s40263-019-00690-8
Pharmacotherapy for Pediatric Convulsive Status Epilepticus
Abstract
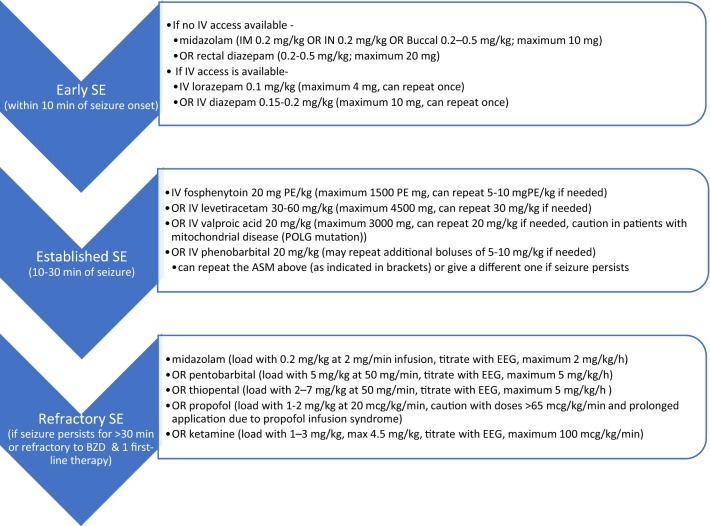
Convulsive status epilepticus (CSE) is one of the most common pediatric neurological emergencies. Ongoing seizure activity is a dynamic process and may be associated with progressive impairment of gamma-aminobutyric acid (GABA)-mediated inhibition due to rapid internalization of GABAA receptors. Further hyperexcitability may be caused by AMPA (alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid) and NMDA (N-methyl-D-aspartic acid) receptors moving from subsynaptic sites to the synaptic membrane. Receptor trafficking during prolonged seizures may contribute to difficulties treating seizures of longer duration and may provide some of the pathophysiological underpinnings of established and refractory SE (RSE). Simultaneously, a practice change toward more rapid initiation of first-line benzodiazepine (BZD) treatment and faster escalation to second-line non-BZD treatment for established SE is in progress. Early administration of the recommended BZD dose is suggested. For second-line treatment, non-BZD anti-seizure medications (ASMs) include valproate, fosphenytoin, or levetiracetam, among others, and at this point there is no clear evidence that any one of these options is better than the others. If seizures continue after second-line ASMs, RSE is manifested. RSE treatment consists of bolus doses and titration of continuous infusions under continuous electro-encephalography (EEG) guidance until electrographic seizure cessation or burst-suppression. Ultimately, etiological workup and related treatment of CSE, including broad spectrum immunotherapies as clinically indicated, is crucial. A potential therapeutic approach for future studies may entail consideration of interventions that may accelerate diagnosis and treatment of SE, as well as rational and early polytherapy based on synergism between ASMs by utilizing medications targeting different mechanisms of epileptogenesis and epileptogenicity.
Conflict of interest statement
Avantika Singh and Coral Stredny have no conflicts of interest or disclosures to report. Tobias Loddenkemper serves on the Council of the American Clinical Neurophysiology Society, on the American Board of Clinical Neurophysiology, as founder and consortium PI of the pediatric status epilepticus research group (pSERG), as an Associate Editor for
Figures
Similar articles
-
Early polytherapy for benzodiazepine-refractory status epilepticus.Epilepsy Behav. 2019 Dec;101(Pt B):106367. doi: 10.1016/j.yebeh.2019.06.011. Epub 2019 Oct 18. Epilepsy Behav. 2019. PMID: 31636007 Review.
-
Treatment of cholinergic-induced status epilepticus with polytherapy targeting GABA and glutamate receptors.Epilepsia Open. 2023 May;8 Suppl 1(Suppl 1):S117-S140. doi: 10.1002/epi4.12713. Epub 2023 Mar 10. Epilepsia Open. 2023. PMID: 36807554 Free PMC article. Review.
-
Benzodiazepine administration patterns before escalation to second-line medications in pediatric refractory convulsive status epilepticus.Epilepsia. 2021 Nov;62(11):2766-2777. doi: 10.1111/epi.17043. Epub 2021 Aug 21. Epilepsia. 2021. PMID: 34418087 Free PMC article.
-
Rational polytherapy in the treatment of cholinergic seizures.Neurobiol Dis. 2020 Jan;133:104537. doi: 10.1016/j.nbd.2019.104537. Epub 2019 Aug 24. Neurobiol Dis. 2020. PMID: 31454548 Review.
-
Early Clinical Variables Associated With Refractory Convulsive Status Epilepticus in Children.Neurology. 2023 Aug 1;101(5):e546-e557. doi: 10.1212/WNL.0000000000207472. Epub 2023 Jun 9. Neurology. 2023. PMID: 37295955 Free PMC article.
Cited by
-
Pharmacotherapy for Nonconvulsive Seizures and Nonconvulsive Status Epilepticus.Drugs. 2021 May;81(7):749-770. doi: 10.1007/s40265-021-01502-4. Epub 2021 Apr 8. Drugs. 2021. PMID: 33830480 Review.
-
Preventing Long-Term Brain Damage by Nerve Agent-Induced Status Epilepticus in Rat Models Applicable to Infants: Significant Neuroprotection by Tezampanel Combined with Caramiphen but Not by Midazolam Treatment.J Pharmacol Exp Ther. 2024 Jan 17;388(2):432-450. doi: 10.1124/jpet.123.001710. J Pharmacol Exp Ther. 2024. PMID: 37739807 Free PMC article.
-
Optimal Management of Status Epilepticus in Children in the Emergency Setting: A Review of Recent Advances.Open Access Emerg Med. 2022 Sep 17;14:491-506. doi: 10.2147/OAEM.S293258. eCollection 2022. Open Access Emerg Med. 2022. PMID: 36158897 Free PMC article. Review.
-
Profile of miRNA expression in the hippocampus of epileptic mice and the prediction of potential therapeutic targets.Mol Biol Rep. 2024 Aug 22;51(1):929. doi: 10.1007/s11033-024-09861-3. Mol Biol Rep. 2024. PMID: 39172288
-
Efficacy and safety of levetiracetam versus valproate in patients with established status epilepticus: A systematic review and meta-analysis.Heliyon. 2023 Feb 1;9(2):e13380. doi: 10.1016/j.heliyon.2023.e13380. eCollection 2023 Feb. Heliyon. 2023. PMID: 36816301 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
