

Current Neurologic Assessment and Neuroprotective Strategies in Cardiac Anesthesia: A Survey to the Membership of the Society of Cardiovascular Anesthesiologists
- PMID: 31880633
- PMCID: PMC7367499
- DOI: 10.1213/ANE.0000000000004601
Current Neurologic Assessment and Neuroprotective Strategies in Cardiac Anesthesia: A Survey to the Membership of the Society of Cardiovascular Anesthesiologists
Abstract
Background: Neurologic injury and cognitive disorder after cardiac surgery are associated with morbidity and mortality. Variability in the application of neuroprotective strategies likely exists during cardiac surgery. The Society of Cardiovascular Anesthesiologists (SCA) conducted a survey among its members on common perioperative neuroprotective strategies: assessment of aortic atheromatous burden, management of intraoperative blood pressure, and use of cerebral oximetry.
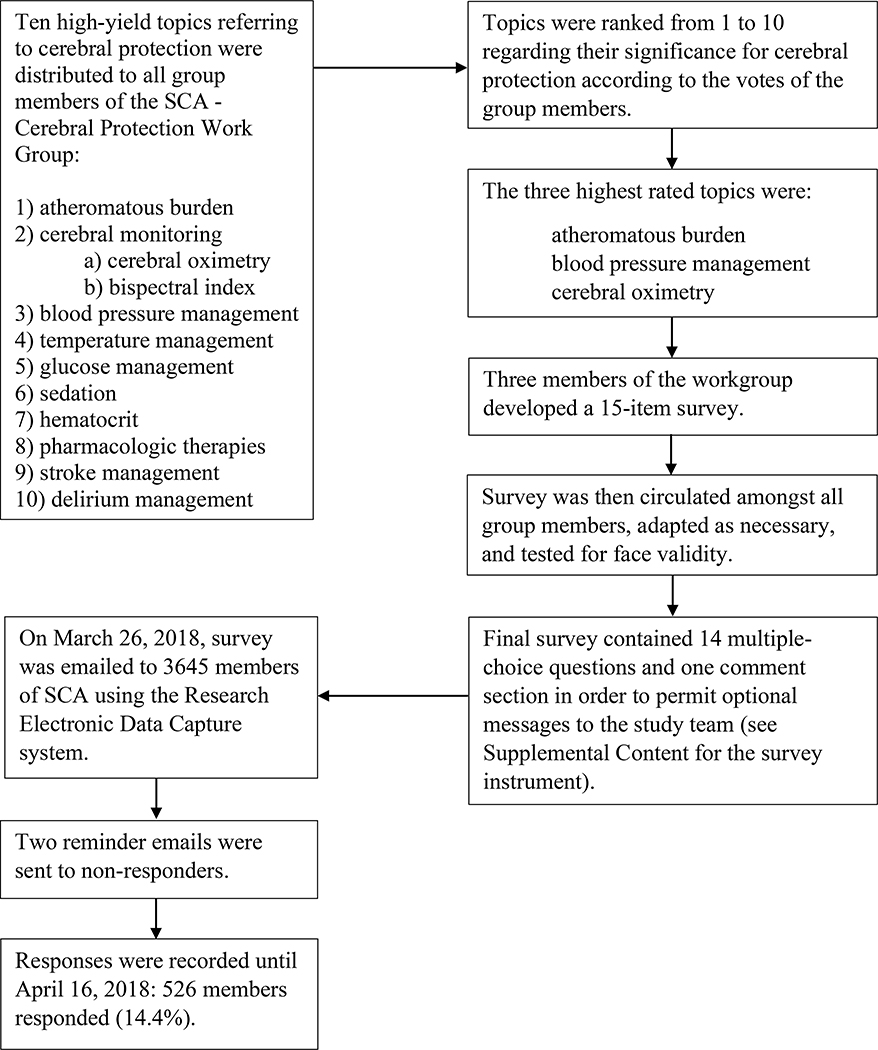
Methods: A 15-item survey was developed by 3 members of the SCA Continuous Practice Improvement - Cerebral Protection Working Group. The questionnaire was then circulated among all working group members, adapted, and tested for face validity. On March 26, 2018, the survey was sent to members of the SCA via e-mail using the Research Electronic Data Capture system. Responses were recorded until April 16, 2018.
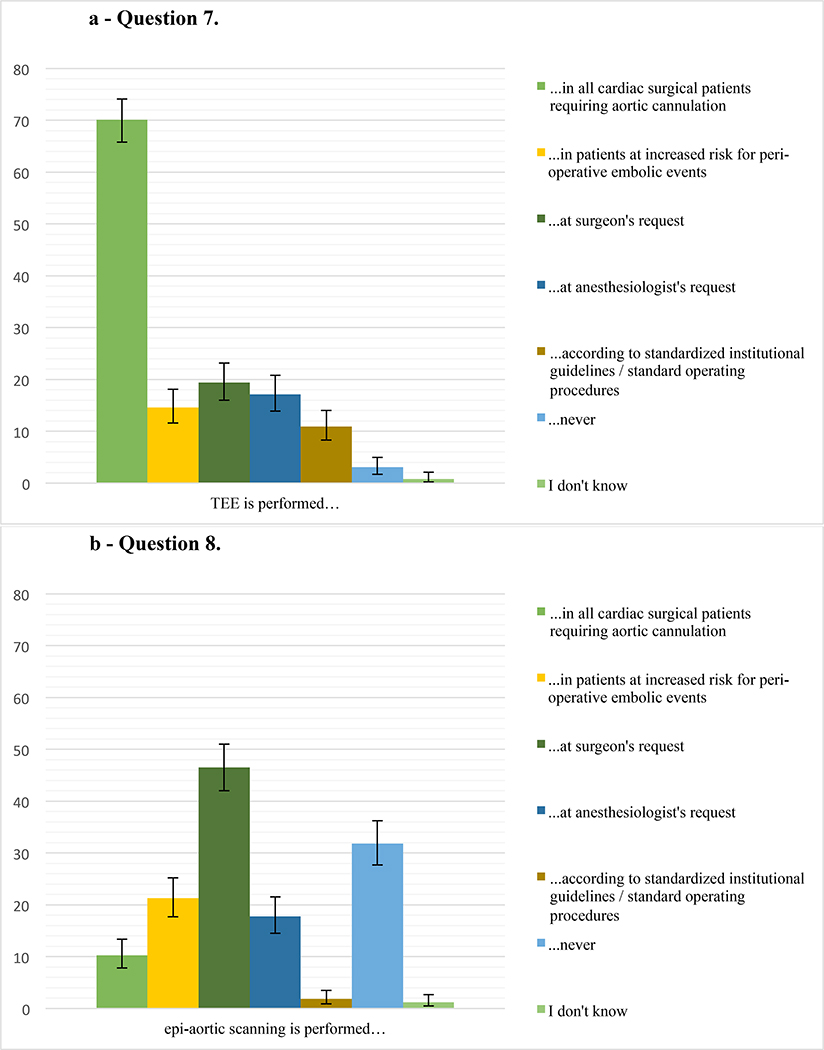
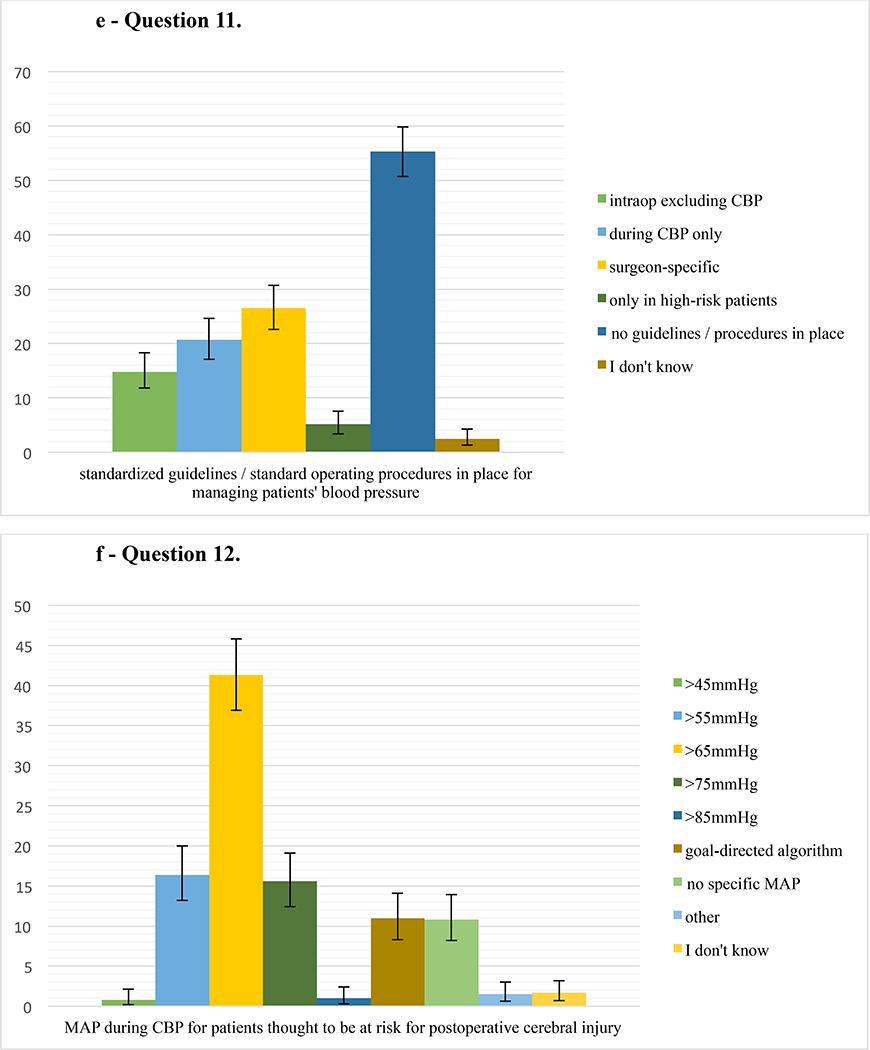
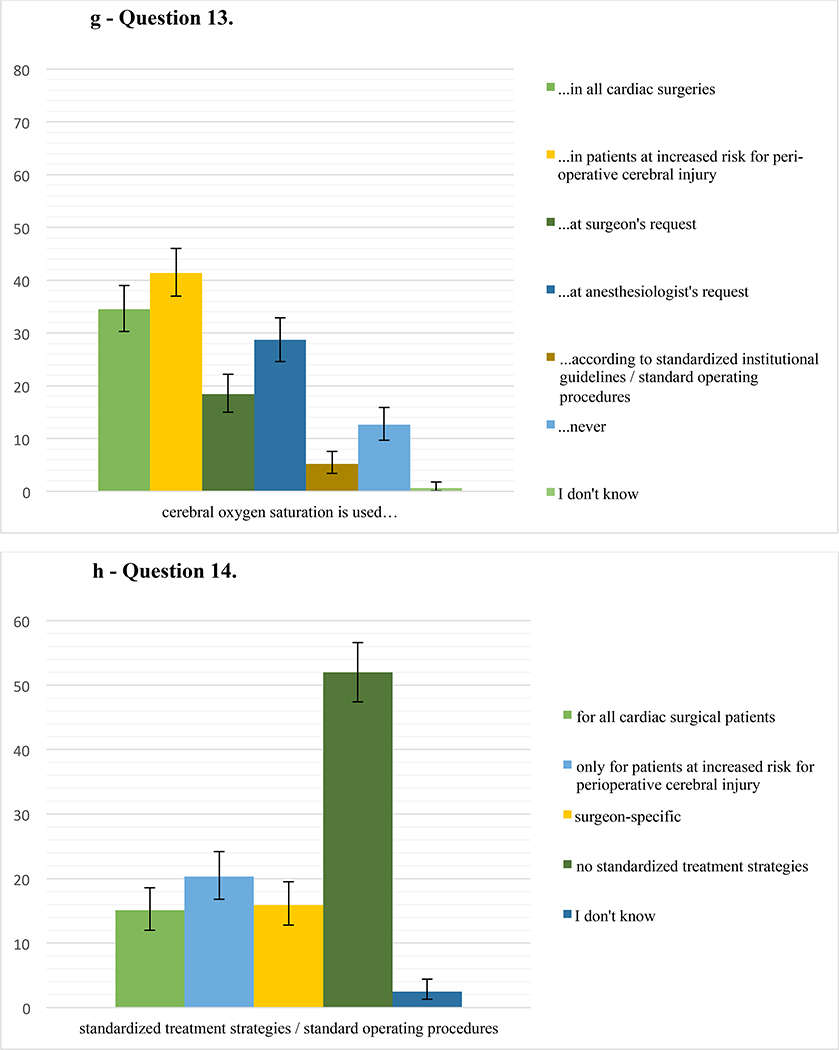
Results: Of the 3645 surveys e-mailed, 526 members responded (14.4%). Most responders worked in academic institutions (58.3%), followed by private practices (38.7%). Epiaortic ultrasound for the assessment of aortic atheromatous burden was most commonly utilized at the surgeon's request (46.5%). Cerebral oximetry was most commonly used in patients with increased perioperative risk of cerebral injury (41.4%). Epiaortic ultrasound (1.9%) and cerebral oximetry (5.2%) were rarely part of a standardized monitoring approach. A majority of respondents (52.0%) reported no standardized management strategies for neuroprotection during cardiac surgery at their institution. A total of 55.3% stated that no standardized institutional guidelines were in place for managing a patient's blood pressure intraoperatively or during cardiopulmonary bypass. When asked about patients at risk for postoperative cerebral injury, 41.3% targeted a blood pressure goal >65 mmHg during cardiopulmonary bypass. The majority of responders (60.4%) who had access to institutional rates of postoperative stroke/cerebral injury had standard neuroprotective strategies in place.
Conclusions: Our data indicate that approximately half of the respondents to this SCA survey do not use standardized guidelines/standard operating procedures for perioperative cerebral protection. The lack of standardized neuroprotective strategies during cardiac surgery may impact postoperative neurologic outcomes. Further investigations are warranted and should assess the association of standardized neuroprotective approaches and postoperative neurological outcomes.
Conflict of interest statement
Figures
References
-
- Gasparovic H, Kopjar T, Rados M et al. Impact of Remote Ischemic Preconditioning Preceding Coronary Artery Bypass Grafting on Inducing Neuroprotection. J Thorac Cardiovasc Surg. 2018. - PubMed
-
- Craver JM, Puskas JD, Weintraub WW et al. 601 Octogenarians Undergoing Cardiac Surgery: Outcome and Comparison with Younger Age Groups. Ann Thorac Surg. 1999;67:1104–10. - PubMed
-
- Newman MF, Kirchner JL, Phillips-Bute B et al. Longitudinal Assessment of Neurocognitive Function after Coronary-Artery Bypass Surgery. N Engl J Med. 2001;344:395–402. - PubMed
-
- Tarakji KG, Sabik JF 3rd, Bhudia SK et al. Temporal Onset, Risk Factors, and Outcomes Associated with Stroke after Coronary Artery Bypass Grafting. JAMA. 2011;305:381–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
