

Patient Views on Religious Institutional Health Care
- PMID: 31880794
- PMCID: PMC6991194
- DOI: 10.1001/jamanetworkopen.2019.17008
Patient Views on Religious Institutional Health Care
Abstract
Importance: Federal protections allow health facilities to limit options to patients on the basis of religious values. Little is known about whether US adults consider religious affiliation when selecting facilities and whether they agree with such limitations.
Objective: To understand patient views on religious institutional care.
Design, setting, and participants: This is a population-based, cross-sectional survey study of US adults recruited from the probability-based AmeriSpeak Omnibus panel available from NORC (formerly the National Opinion Research Center) at the University of Chicago. Surveys were administered via internet or telephone during a 3-day fielding period in November 2017. Data analysis was performed from January 2018 to October 2019.
Exposures: Participant characteristics, including religiosity measures.
Main outcomes and measures: Whether patients consider religious affiliation when selecting a health care facility and their views on whether an institution's religious values should take precedence over their health choices. Responses were compared by gender. When gender differences existed, regression models were performed, and thematic content analysis was applied to open-ended responses.
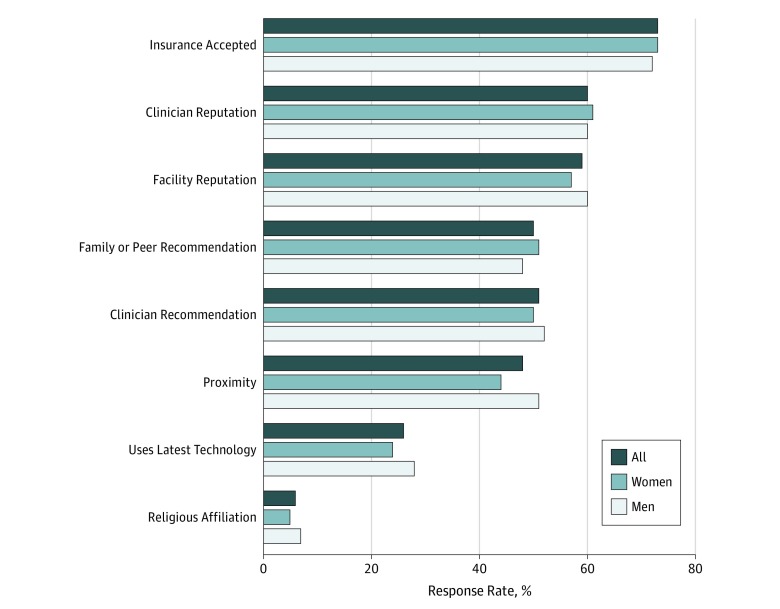
Results: There were 1446 participants (745 [51.5%] male; mean [SD] age, 46 [17] years), for a survey completion rate of 24.5% and weighted cumulative response weight of 7.3%. Most respondents (62.6%) were white, and the most common religion was Protestant (28.2%). When specifically asked, only 6.4% reported that they considered religious affiliation when selecting a health care facility; most participants (71.3%) reported when selecting a health care facility that they did not care whether it is religiously affiliated, 13.4% preferred a religious affiliation, and 15.3% preferred no religious affiliation. There were no gender differences. Most participants (71.4%) believed that their health choices should take priority over an institution's religious affiliation in services offered, and this was more common for women than for men (74.9% vs 68.1%; difference, 6.8%; 95% CI, 5.6%-8.2%; P = .005), who more commonly endorsed concerns for personal choice and autonomy over one's own body.
Conclusions and relevance: This study suggests that most patients value their personal choices, yet do not consider an institution's religious affiliation when choosing their source of health care. Women placed greater emphasis on their autonomy in comparison with an institution's right to invoke religious restrictions to care. Given the growth in ownership of health care facilities by religious entities in the United States and increasing attention to conscientious objections, these findings point to a need for advocacy and legislation that effectively balances protections for religious institutions with protections for patients.
Conflict of interest statement
Figures
Comment in
-
On the Opinions of US Adults Regarding Religiously Affiliated Health Care Facilities.JAMA Netw Open. 2019 Dec 2;2(12):e1919013. doi: 10.1001/jamanetworkopen.2019.19013. JAMA Netw Open. 2019. PMID: 31880789 No abstract available.
Similar articles
-
Religious hospital policies on reproductive care: what do patients want to know?Am J Obstet Gynecol. 2018 Feb;218(2):251.e1-251.e9. doi: 10.1016/j.ajog.2017.11.595. Epub 2017 Dec 6. Am J Obstet Gynecol. 2018. PMID: 29221943
-
Religious affiliations and consumer behavior: an examination of hospitals.J Health Care Mark. 1993 Winter;13(4):42-9. J Health Care Mark. 1993. PMID: 10131733
-
Religious hospitals and primary care physicians: conflicts over policies for patient care.J Gen Intern Med. 2010 Jul;25(7):725-30. doi: 10.1007/s11606-010-1329-6. Epub 2010 Apr 6. J Gen Intern Med. 2010. PMID: 20373045 Free PMC article.
-
Varieties of Religious (Non)Affiliation: A Primer for Mental Health Practitioners on the "Spiritual but Not Religious" and the "Nones".J Nerv Ment Dis. 2020 May;208(5):424-430. doi: 10.1097/NMD.0000000000001141. J Nerv Ment Dis. 2020. PMID: 32282550 Review.
-
The role of religious values in decisions about genetics and the public's health.J Relig Health. 2014 Jun;53(3):702-14. doi: 10.1007/s10943-013-9814-y. J Relig Health. 2014. PMID: 24510076 Review.
Cited by
-
Patient Perspectives on Religiously Affiliated Care in Rural and Urban Colorado.J Prim Care Community Health. 2021 Jan-Dec;12:21501327211012158. doi: 10.1177/21501327211012158. J Prim Care Community Health. 2021. PMID: 33949248 Free PMC article.
-
National variability in Americans' COVID-19 protective behaviors: Implications for vaccine roll-out.PLoS One. 2021 Nov 5;16(11):e0259257. doi: 10.1371/journal.pone.0259257. eCollection 2021. PLoS One. 2021. PMID: 34739498 Free PMC article.
-
Managing Spiritual Care Departments During the COVID-19 Pandemic: A Qualitative Study.J Pastoral Care Counsel. 2022 Dec;76(4):294-303. doi: 10.1177/15423050221122029. Epub 2022 Oct 11. J Pastoral Care Counsel. 2022. PMID: 36217802 Free PMC article.
-
Religious Hospitals and Poorer Health Outcomes: A Case Study Using Hospital Performance Ratings.Inquiry. 2025 Jan-Dec;62:469580251350813. doi: 10.1177/00469580251350813. Epub 2025 Jun 24. Inquiry. 2025. PMID: 40552389 Free PMC article.
-
Gender-Affirming Surgery Price Transparency and Online Information Availability in US Hospitals.Aesthetic Plast Surg. 2025 Jun 24. doi: 10.1007/s00266-025-05017-1. Online ahead of print. Aesthetic Plast Surg. 2025. PMID: 40555740
References
-
- Uttley L, Khaikin C Growth of catholic hospitals and health systems: 2016 update of the miscarriage of medicine report. http://static1.1.sqspcdn.com/static/f/816571/27061007/1465224862580/MW_U.... Published 2016. Accessed June 28, 2019.
-
- US Conference of Catholic Bishops Ethical and religious directives for Catholic health care services. 6th ed. http://www.usccb.org/about/doctrine/ethical-and-religious-directives/upl.... Published 2018. Accessed June 28, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
