

The use of biologic therapies for the management of pediatric asthma
- PMID: 31880870
- PMCID: PMC7018587
- DOI: 10.1002/ppul.24613
The use of biologic therapies for the management of pediatric asthma
Abstract
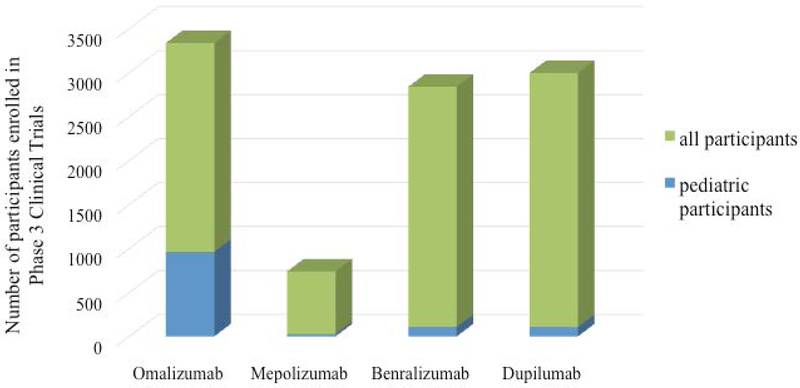
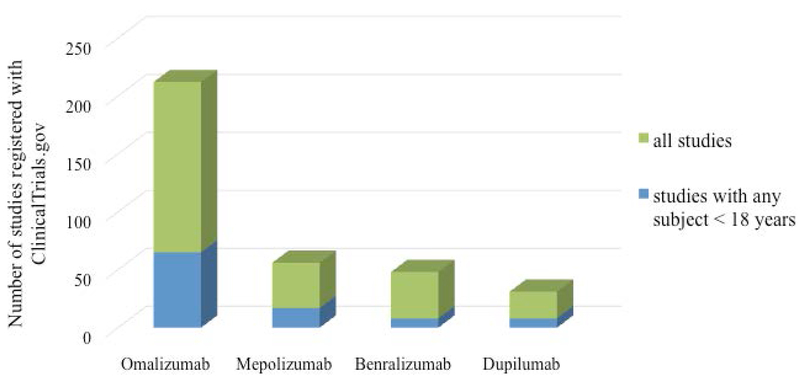
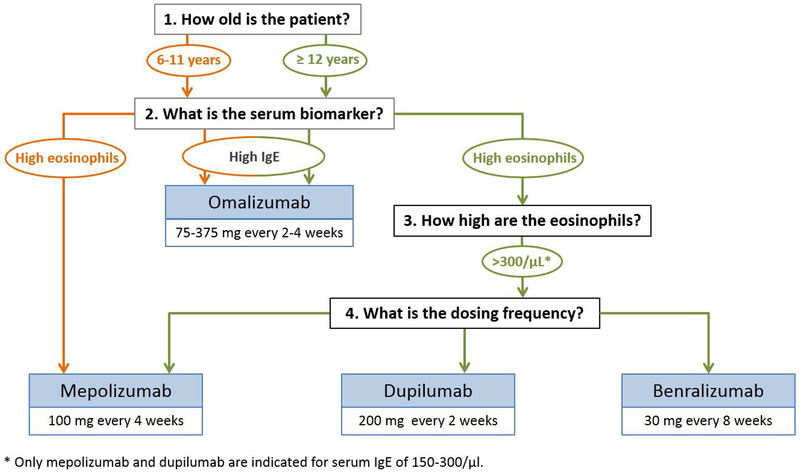
With better understanding of the role of type 2 inflammation in allergic asthma, there has been progress made in the development of new biologic therapies targeting these specific pathways. This review will consider diagnostic criteria for using biologic therapies for pediatric asthma with special emphasis on populations that are likely to benefit the most from particular therapies. With the exception of the anti-immunoglobulin E, omalizumab, very few studies have been published on the efficacy and safety of biologic therapies in children, particularly anti-interleukin-5 (IL5) and anti-IL4/IL13 therapies. The review will highlight the scarcity of published data in pediatric-specific populations. In addition, we will consider the cost-effectiveness as well as potential long-term consequences of biologic therapies in pediatric asthma.
Keywords: T-helper 2 asthma; anti-IgE therapy; anti-eosinophil therapy; childhood asthma; monoclonal antibodies.
© 2019 Wiley Periodicals, Inc.
Figures
References
-
- Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. 2012; 5:716–25. - PubMed
-
- Schatz M and Rosenwasser L. The allergic asthma phenotype. J Allergy Clin Immunol Pract. 2014; 6:645–8; quiz 49. - PubMed
-
- Holgate ST and Polosa R. Treatment strategies for allergy and asthma. Nat Rev Immunol. 2008; 3:218–30. - PubMed
