

Phase III Study of Adjuvant Ipilimumab (3 or 10 mg/kg) Versus High-Dose Interferon Alfa-2b for Resected High-Risk Melanoma: North American Intergroup E1609
- PMID: 31880964
- PMCID: PMC7030886
- DOI: 10.1200/JCO.19.01381
Phase III Study of Adjuvant Ipilimumab (3 or 10 mg/kg) Versus High-Dose Interferon Alfa-2b for Resected High-Risk Melanoma: North American Intergroup E1609
Abstract
Purpose: Phase III adjuvant trials have reported significant benefits in both relapse-free survival (RFS) and overall survival (OS) for high-dose interferon alfa (HDI) and ipilimumab at 10 mg/kg (ipi10). E1609 evaluated the safety and efficacy of ipilimumab at 3 mg/kg (ipi3) and ipi10 versus HDI.
Patients and methods: E1609 was a phase III trial in patients with resected cutaneous melanoma (American Joint Committee on Cancer 7th edition stage IIIB, IIIC, M1a, or M1b). It had 2 coprimary end points: OS and RFS. A 2-step hierarchic approach first evaluated ipi3 versus HDI followed by ipi10 versus HDI.
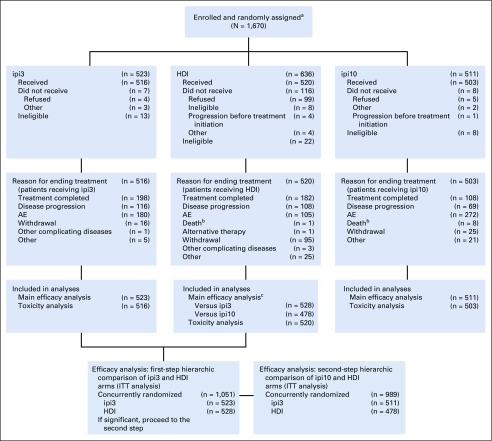
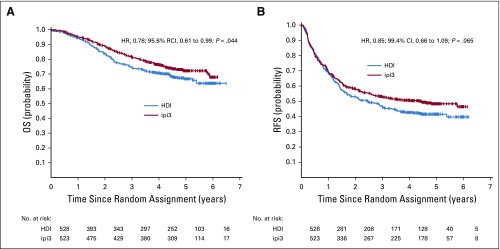
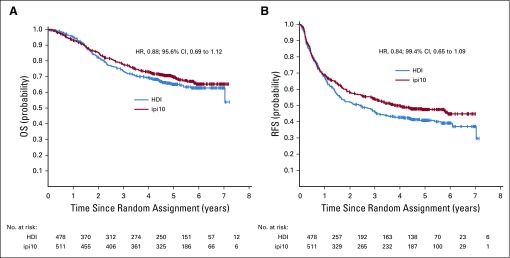
Results: Between May 2011 and August 2014, 1,670 adult patients were centrally randomly assigned (1:1:1) to ipi3 (n = 523), HDI (n = 636), or ipi10 (n = 511). Treatment-related adverse events grade ≥ 3 occurred in 37% of patients receiving ipi3, 79% receiving HDI, and 58% receiving ipi10, with adverse events leading to treatment discontinuation in 35%, 20%, and 54%, respectively. Comparison of ipi3 versus HDI used an intent-to-treat analysis of concurrently randomly assigned patient cases (n = 1,051) and showed significant OS difference in favor of ipi3 (hazard ratio [HR], 0.78; 95.6% repeated CI, 0.61 to 0.99; P = .044; RFS: HR, 0.85; 99.4% CI, 0.66 to 1.09; P = .065). In the second step, for ipi10 versus HDI (n = 989), trends in favor of ipi10 did not achieve statistical significance. Salvage patterns after melanoma relapse showed significantly higher rates of ipilimumab and ipilimumab/anti-programmed death 1 use in the HDI arm versus ipi3 and ipi10 (P ≤ .001).
Conclusion: Adjuvant therapy with ipi3 benefits survival versus HDI; for the first time to our knowledge in melanoma adjuvant therapy, E1609 has demonstrated a significant improvement in OS against an active control regimen. The currently approved adjuvant ipilimumab dose (ipi10) was more toxic and not superior in efficacy to HDI.
Conflict of interest statement
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, nor does mention of trade names, commercial products, or organizations imply endorsement by the US government.
Figures
Comment in
-
Another Victory for Immune Checkpoint Blockade in Melanoma: Adjuvant Ipilimumab Over Interferon.J Clin Oncol. 2020 Feb 20;38(6):529-531. doi: 10.1200/JCO.19.02988. Epub 2019 Dec 27. J Clin Oncol. 2020. PMID: 31880967 No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Kirkwood JM, Strawderman MH, Ernstoff MS, et al. Interferon alfa-2b adjuvant therapy of high-risk resected cutaneous melanoma: The Eastern Cooperative Oncology Group trial EST 1684. J Clin Oncol. 1996;14:7–17. - PubMed
-
- Eggermont AM, Suciu S, Testori A, et al. Long-term results of the randomized phase III trial EORTC 18991 of adjuvant therapy with pegylated interferon alfa-2b versus observation in resected stage III melanoma. J Clin Oncol. 2012;30:3810–3818. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA180802/CA/NCI NIH HHS/United States
- U10 CA180847/CA/NCI NIH HHS/United States
- UG1 CA233373/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180835/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- UG1 CA233277/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- UG1 CA233163/CA/NCI NIH HHS/United States
- U10 CA180799/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180853/CA/NCI NIH HHS/United States
- U10 CA180844/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
