

Improving accuracy for finite element modeling of endovascular coiling of intracranial aneurysm
- PMID: 31881029
- PMCID: PMC6934293
- DOI: 10.1371/journal.pone.0226421
Improving accuracy for finite element modeling of endovascular coiling of intracranial aneurysm
Abstract
Background: Computer modeling of endovascular coiling intervention for intracranial aneurysm could enable a priori patient-specific treatment evaluation. To that end, we previously developed a finite element method (FEM) coiling technique, which incorporated simplified assumptions. To improve accuracy in capturing real-life coiling, we aimed to enhance the modeling strategies and experimentally test whether improvements lead to more accurate coiling simulations.
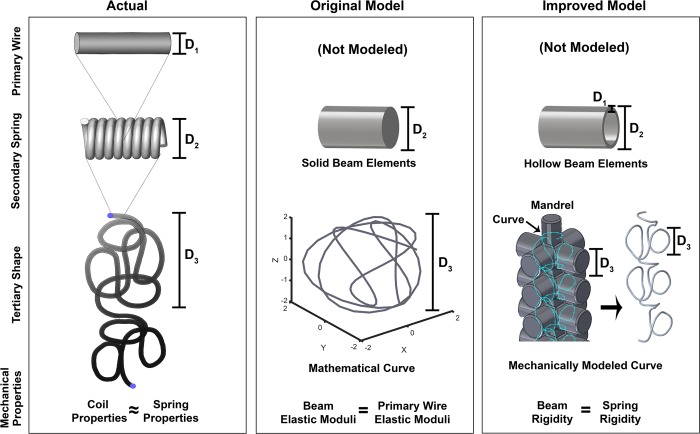
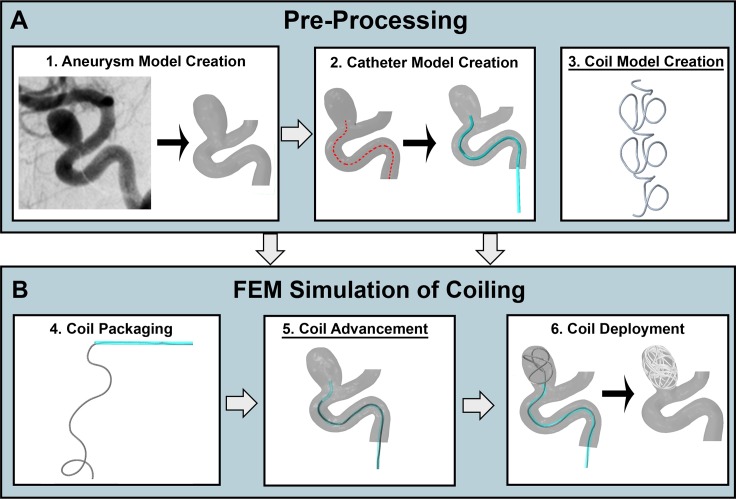
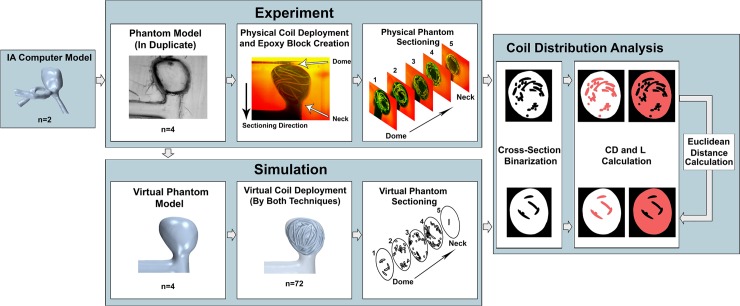
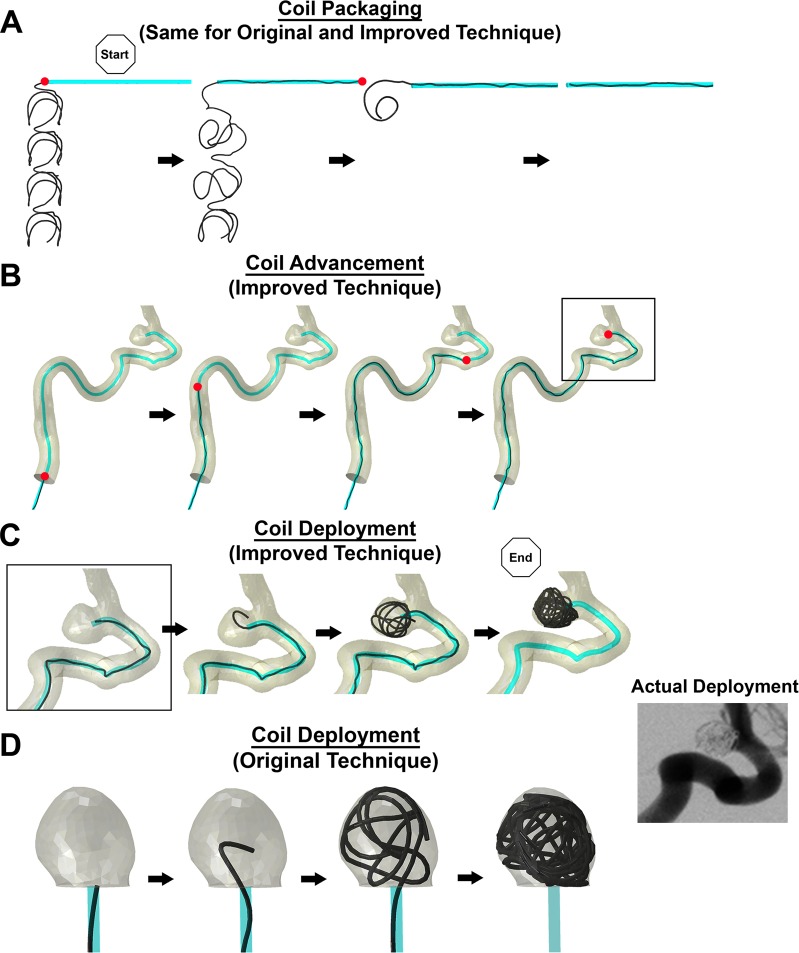
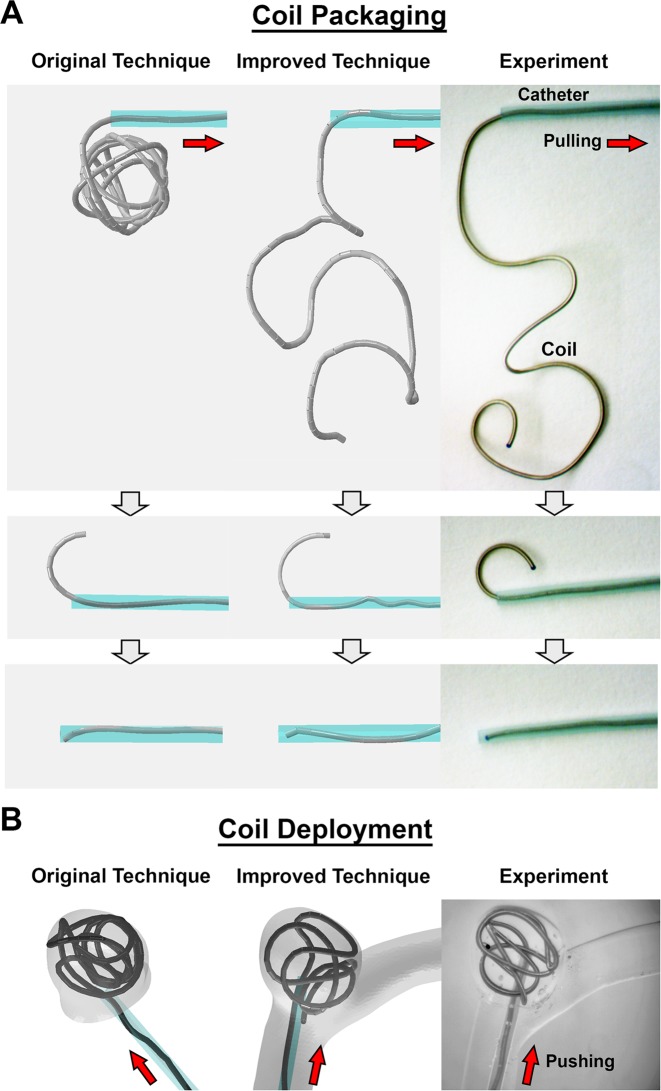
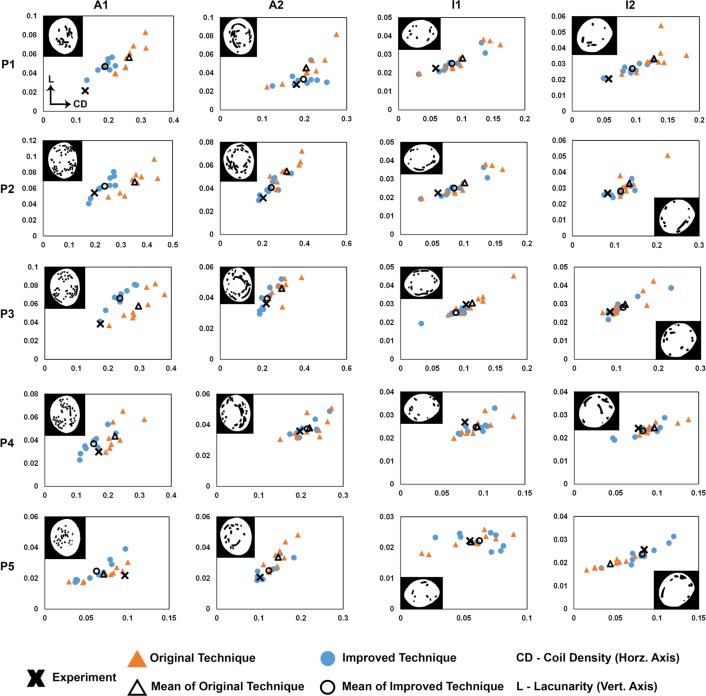
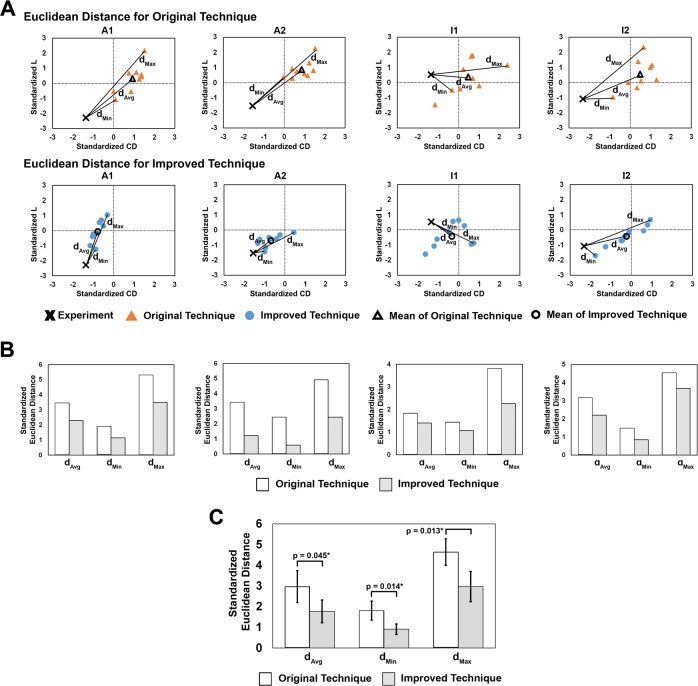
Methods: We previously modeled coils using a pre-shape based on mathematical curves and mechanical properties based on those of platinum wires. In the improved version, to better represent the physical properties of coils, we model coil pre-shapes based on how they are manufactured, and their mechanical properties based on their spring-like geometric structures. To enhance the deployment mechanics, we include coil advancement to the aneurysm in FEM simulations. To test if these new strategies produce more accurate coil deployments, we fabricated silicone phantoms of 2 patient-specific aneurysms in duplicate, deployed coils in each, and quantified coil distributions from intra-aneurysmal cross-sections using coil density (CD) and lacunarity (L). These deployments were simulated 9 times each using the original and improved techniques, and CD and L were calculated for cross-sections matching those in the experiments. To compare the 2 simulation techniques, Euclidean distances (dMin, dMax, and dAvg) between experimental and simulation points in standardized CD-L space were evaluated. Univariate tests were performed to determine if these distances were significantly different between the 2 simulations.
Results: Coil deployments using the improved technique agreed better with experiments than the original technique. All dMin, dMax, and dAvg values were smaller for the improved technique, and the average values across all simulations for the improved technique were significantly smaller than those from the original technique (dMin: p = 0.014, dMax: p = 0.013, dAvg: p = 0.045).
Conclusion: Incorporating coil-specific physical properties and mechanics improves accuracy of FEM simulations of endovascular intracranial aneurysm coiling.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: RJD – None; VMT – Co-founder: Neurovascular Diagnostics, Inc.; SRL – None; NP – None; GFD – None; JMD – Stock/Stock Options: Rist Neurovascular, Inc.; Consultancy: Cerevenous, Medtronic; Payment for Lectures Including Service on Speakers Bureaus: Penumbra; AHS – Financial Interest/Investor/Stock Options/Ownership: Amnis Therapeutics, Apama Medical, BlinkTBI, Inc, Buffalo Technology Partners, Inc., Cardinal Health, Cerebrotech Medical Systems, Inc, Claret Medical, Cognition Medical, Endostream Medical, Ltd, Imperative Care, International Medical Distribution Partners, Rebound Therapeutics Corp., Silk Road Medical, StimMed, Synchron, Three Rivers Medical, Inc., Viseon Spine, Inc. Consultant/Advisory Board: Amnis Therapeutics, Boston Scientific, Canon Medical Systems USA, Inc., Cerebrotech Medical Systems, Inc., Cerenovus, Claret Medical, Corindus, Inc., Endostream Medical, Ltd, Guidepoint Global Consulting, Imperative Care, Integra, Medtronic, MicroVention, Northwest University – DSMB Chair for HEAT Trial, Penumbra, Rapid Medical, Rebound Therapeutics Corp., Silk Road Medical, StimMed, Stryker, Three Rivers Medical, Inc., VasSol, W.L. Gore & Associates. National PI/Steering Committees: Cerenovus LARGE Trial and ARISE II Trial, Medtronic SWIFT PRIME and SWIFT DIRECT Trials, MicroVention FRED Trial & CONFIDENCE Study, MUSC POSITIVE Trial, Penumbra 3D Separator Trial, COMPASS Trial, INVEST Trial. HM – Co-founder: Neurovascular Diagnostics, Inc. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366(9488):809–17. 10.1016/S0140-6736(05)67214-5 . - DOI - PubMed
-
- Damiano RJ, Ma D, Xiang J, Siddiqui AH, Snyder KV, Meng H. Finite element modeling of endovascular coiling and flow diversion enables hemodynamic prediction of complex treatment strategies for intracranial aneurysm. Journal of biomechanics. 2015;48(12):3332–40. 10.1016/j.jbiomech.2015.06.018 . - DOI - PMC - PubMed
-
- Otani T, Ii S, Shigematsu T, Fujinaka T, Hirata M, Ozaki T, et al. Computational model of coil placement in cerebral aneurysm with using realistic coil properties. Journal of Biomechanical Science and Engineering. 2015;10(4):15-00555-15-. 10.1299/jbse.15-00555 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
