

Mento's change model in teaching competency-based medical education
- PMID: 31882006
- PMCID: PMC6935174
- DOI: 10.1186/s12909-019-1896-0
Mento's change model in teaching competency-based medical education
Abstract
Background: Resistance to change is customary and is expected in any organization. However, most of the downsides of change can be avoided if the organization/individual prepares for the change by acknowledging guided strategies. In healthcare, change is the state of nature, which has also translated to medical education (ME). ME in the current era has undergone a shift from a traditional content-based curriculum to a competency-based curriculum. Recently, however, the broader social-accountability movement has accelerated this rate of transformation. One of the key challenges to educators harbingering this transformation to competency-based medical education (CBME) is to redesign the processes of teaching.
Aim: Here we define a framework designed using Mento's model of change that will totally agree with introducing positive change in teaching in an institution undergoing transformation from a traditional content-based curriculum to a competency-based curriculum.
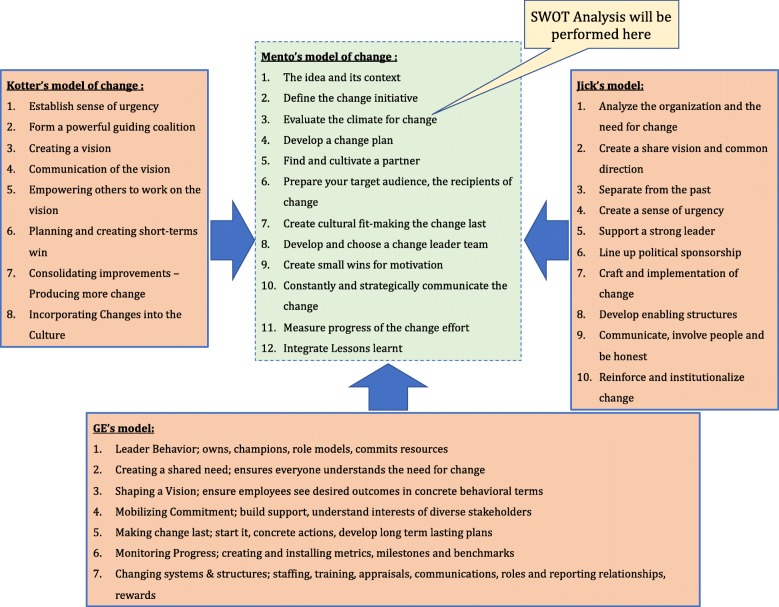
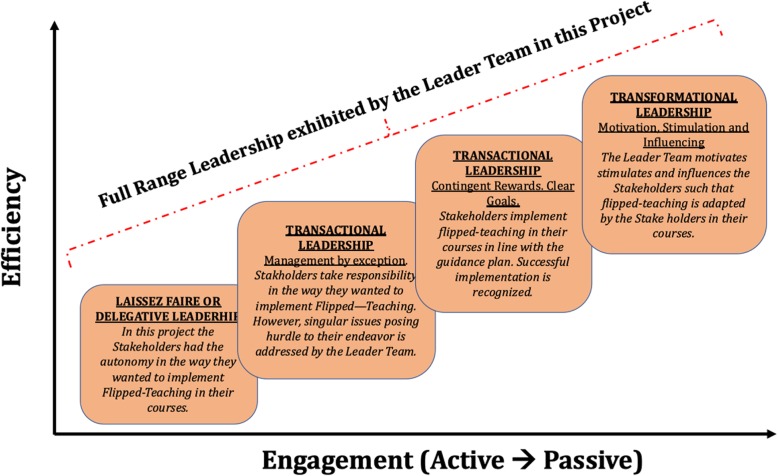
Methodology: Using Schein's "unfreezing" as a guide term we critically reflected on the popular change-management models, to home in on Kotter's model of change to transform organizations. However, Kotter's change-model draws from Situational and Contingency Leadership Theories, which may not agree with academic organizations involved in ME. As such organizations adhere to Transactional and Transformational Leadership archetypes, where Leadership is constructively executed by "The Leader Team", we decided to adopt Mento's change-model for our study. Mento's model not only draws from the precepts of Kotter's model, but also incorporates axioms of Jick's and GE's change-models.
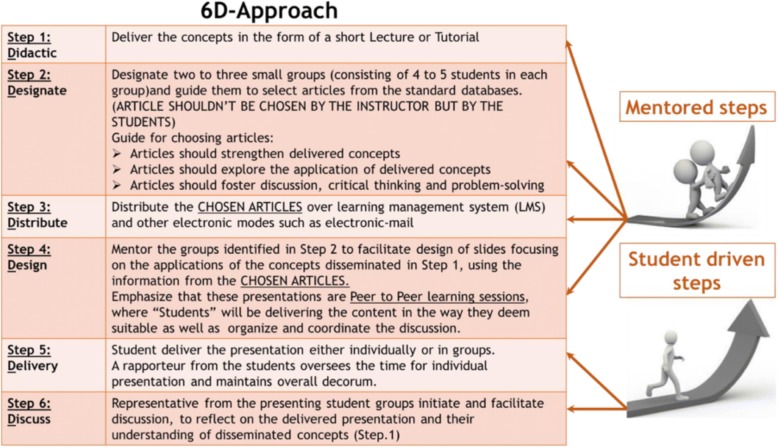
Results: Using Mento's model a framework was blueprinted to implement active learning (AL) strategies in CBME. Here we have elaborated on the framework using the exemplar of flipped teaching. The development of this framework required the design and execution of a faculty development program, and a step by step guidance plan to chaperon, instruct and implement change in teaching to harbinger CBME. Further, we have also reflected on the change process using Gravin's framework.
Conclusion: To our knowledge this is the first report of the use of Mento's model of change in medical education. Also, the blueprinted framework is supported by acknowledged leadership theories and can be translated to implement any curricular change in CBME.
Keywords: 6D-approach; Active learning; Change-management; Competency based medical education; Flipped-teaching; Kotter’s model of change; Leadership theory; Mento’s model of change.
Figures
Similar articles
-
Confronting the Challenges of Anatomy Education in a Competency-Based Medical Curriculum During Normal and Unprecedented Times (COVID-19 Pandemic): Pedagogical Framework Development and Implementation.JMIR Med Educ. 2020 Oct 7;6(2):e21701. doi: 10.2196/21701. JMIR Med Educ. 2020. PMID: 32873536 Free PMC article.
-
Implementing competency-based medical education: What changes in curricular structure and processes are needed?Med Teach. 2017 Jun;39(6):594-598. doi: 10.1080/0142159X.2017.1315077. Med Teach. 2017. PMID: 28598748
-
Implementation of United Arab Emirates competency framework for medical education in undergraduate medical curriculum.BMC Med Educ. 2025 May 27;25(1):782. doi: 10.1186/s12909-025-07342-0. BMC Med Educ. 2025. PMID: 40426128 Free PMC article.
-
Curriculum reform for residency training: competence, change, and opportunities for leadership.Can J Anaesth. 2016 Jul;63(7):875-84. doi: 10.1007/s12630-016-0637-7. Epub 2016 Apr 4. Can J Anaesth. 2016. PMID: 27044399 Review. English.
-
Assessment to transform competency-based curricula.Am J Pharm Educ. 2009 Dec 17;73(8):158. doi: 10.5688/aj7308158. Am J Pharm Educ. 2009. PMID: 20221351 Free PMC article. Review.
Cited by
-
Confronting the Challenges of Anatomy Education in a Competency-Based Medical Curriculum During Normal and Unprecedented Times (COVID-19 Pandemic): Pedagogical Framework Development and Implementation.JMIR Med Educ. 2020 Oct 7;6(2):e21701. doi: 10.2196/21701. JMIR Med Educ. 2020. PMID: 32873536 Free PMC article.
-
Students' Perception of Formative Assessment as an Instructional Tool in Competency-Based Medical Education: Proposal for a Proof-of-Concept Study.JMIR Res Protoc. 2023 Mar 20;12:e41626. doi: 10.2196/41626. JMIR Res Protoc. 2023. PMID: 36939831 Free PMC article.
-
Change Management in Medical Contexts, especially in Medical Education: A Systematized Review.J Adv Med Educ Prof. 2022 Oct;10(4):219-227. doi: 10.30476/JAMP.2022.96519.1704. J Adv Med Educ Prof. 2022. PMID: 36310665 Free PMC article. Review.
-
Encouraging students' engagement and promoting deep learning in immunology through an interactive clinical case problem-solving (CCPS) approach: Perception among cohort of medical students in Oman.J Educ Health Promot. 2022 Dec 28;11:410. doi: 10.4103/jehp.jehp_162_22. eCollection 2022. J Educ Health Promot. 2022. PMID: 36824098 Free PMC article.
-
Progressive muscle relaxation in pandemic times: bolstering medical student resilience through IPRMP and Gagne's model.Front Psychol. 2024 Mar 13;15:1240791. doi: 10.3389/fpsyg.2024.1240791. eCollection 2024. Front Psychol. 2024. PMID: 38544521 Free PMC article.
References
-
- Kotter J, Cohen D. The heart of change. Boston: Harvard Business Review Press; 2002.
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
