

Rectosigmoidal manifestations of venous malformations: MR imaging findings and interdisciplinary therapeutic modalities
- PMID: 31882623
- PMCID: PMC6934467
- DOI: 10.1038/s41598-019-56217-0
Rectosigmoidal manifestations of venous malformations: MR imaging findings and interdisciplinary therapeutic modalities
Erratum in
-
Author Correction: Rectosigmoidal manifestations of venous malformations: MR imaging findings and interdisciplinary therapeutic modalities.Sci Rep. 2020 Feb 7;10(1):2458. doi: 10.1038/s41598-020-59025-z. Sci Rep. 2020. PMID: 32034240 Free PMC article.
Abstract
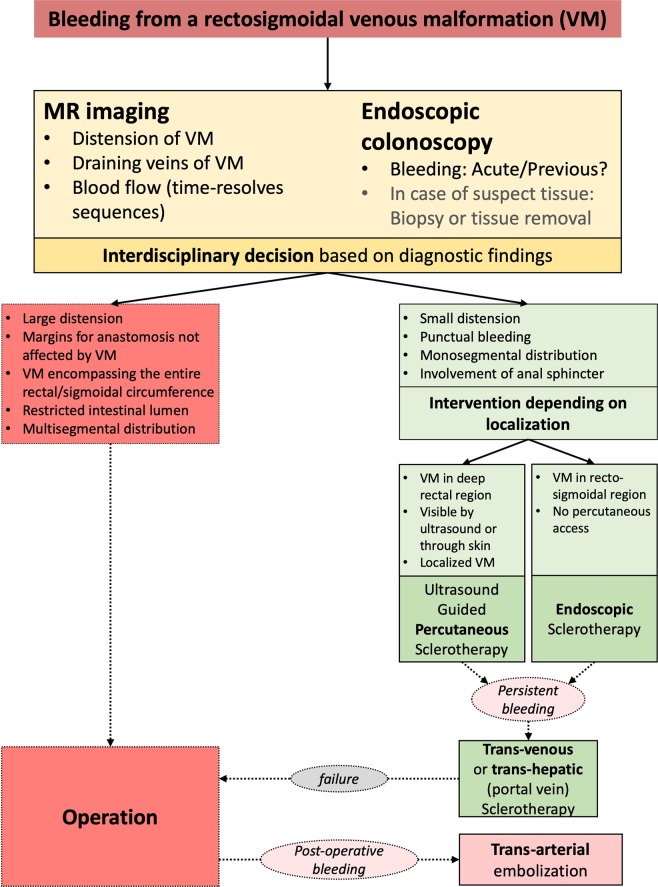
The aim of this study was to identify the frequency of rectosigmoidal involvement in patients with venous malformations (VM) of the lower extremities and to demonstrate multidisciplinary therapeutic options. The medical records and magnetic resonance images (MRI) of patients with VM of the lower extremities, over a six-year period, were reviewed retrospectively in order to determine the occurrence of rectosigmoidal involvement. Vascular interventions, surgical treatments, percutaneous and hybrid (endoscopy-guided angiography) sclerotherapy and procedural complications (according to Clavien-Dindo classification) were also noted. Of the 378 patients with vascular malformation of the lower limbs, 19 patients (5%) had documented venous rectosigmoidal malformation. All of these 19 patients reported episodes of rectal bleeding, while seven patients (36.8%) also had anemia. All patients underwent endoscopy. By endoscopy, seven patients (36.8%) showed discreet changes, and 12 patients (63.2%) showed pronounced signs of submucosal VM with active (47.3%) or previous (15.7%) bleeding. Treatment was performed in all patients with pronounced findings. Six patients underwent endoscopy-guided hybrid sclerotherapy, one patient underwent endoscopic tissue removal, one patient received percutaneous sclerotherapy and one patient received a combination of transvenous embolization and hybrid sclerotherapy. Three patients required open surgery. No complications occurred after conservative treatments; however, one complication was reported after open surgery. None of the treated patients reported further bleeding and anemia at the end of the follow-up period. In this cohort, rectosigmoidal VM occurred in 5% of patients presenting with a high incidence of rectal bleeding. Percutaneous or endoscopy-guided hybrid sclerotherapy appeared to be a safe and effective alternative to surgery.
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Fishman SJ, Fox VL. Visceral vascular anomalies. Gastrointest Endosc Clin N Am. 2001;11(813–834):viii. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
