

Early postoperative weight gain is associated with increased risk of graft failure in living donor liver transplant recipients
- PMID: 31882790
- PMCID: PMC6934543
- DOI: 10.1038/s41598-019-56543-3
Early postoperative weight gain is associated with increased risk of graft failure in living donor liver transplant recipients
Abstract
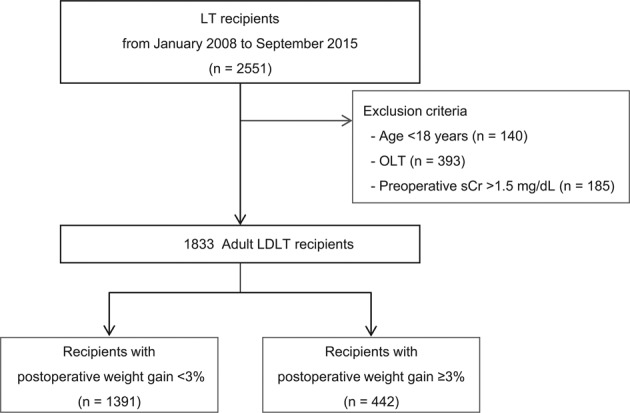
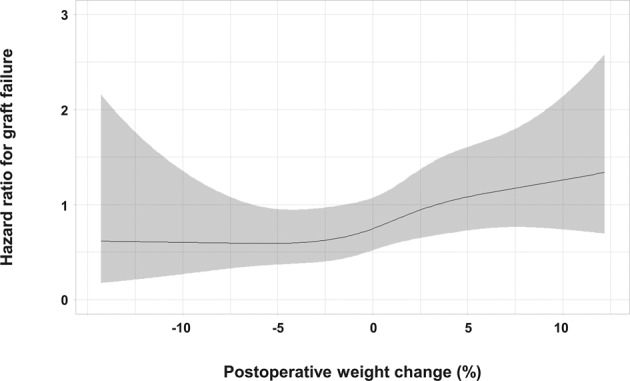
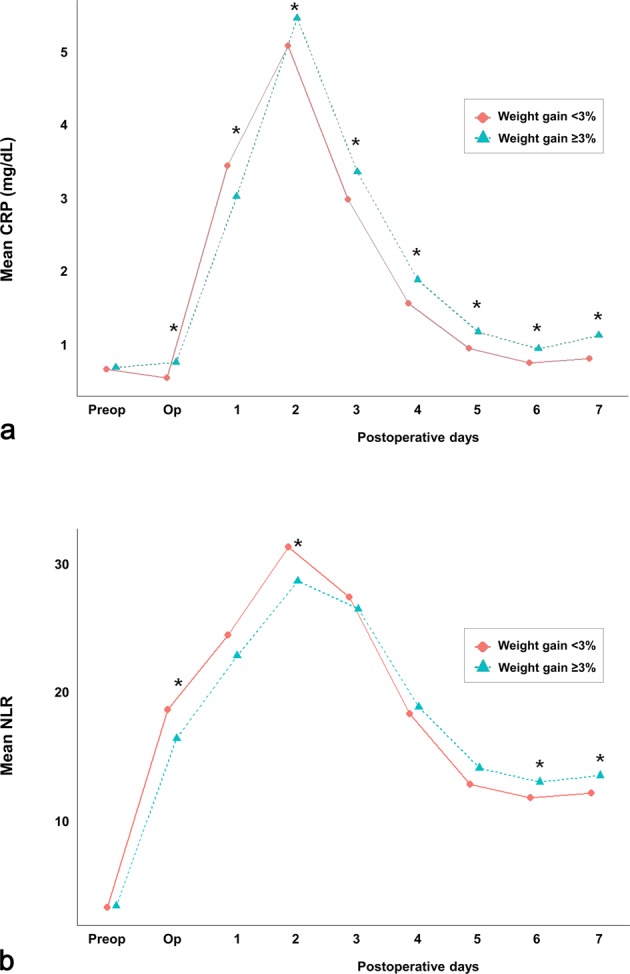
Fluid overload (FO) has been shown to adversely affect multiple organs and survival in critically ill patients. Liver transplantation (LT) carries the risk of massive transfusion, which frequently results in FO. We investigated the association of postoperative weight gain with graft failure, early allograft dysfunction (EAD), and overall mortality in LT. 1833 living donor LT (LDLT) recipients were retrospectively analysed. Patients were divided into 2 groups according to postoperative weight gain (<3% group [n = 1391] and ≥3% group [n = 442]) by using maximally selected log-rank statistics for graft failure. Multivariate Cox and logistic regression analyses were performed. The ≥3% group was associated with graft failure (adjusted HR [aHR], 1.763; 95% CI, 1.248-2.490; P = 0.001). When postoperative weight change was used as a continuous variable, the aHR for each 1% increase in postoperative weight was 1.045 (95% CI, 1.009-1.082; P = 0.015). In addition, the ≥3% group was associated with EAD (adjusted OR [aOR], 1.553; 95% CI, 1.024-2.356; P = 0.038) and overall mortality (aHR, 1.731; 95% CI, 1.182-2.535; P = 0.005). In conclusion, postoperative weight gain may be independently associated with increased risk of graft failure, EAD, and mortality in LDLT recipients.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
