

Patterns of distant metastases in 215 Merkel cell carcinoma patients: Implications for prognosis and surveillance
- PMID: 31883234
- PMCID: PMC7013053
- DOI: 10.1002/cam4.2781
Patterns of distant metastases in 215 Merkel cell carcinoma patients: Implications for prognosis and surveillance
Abstract
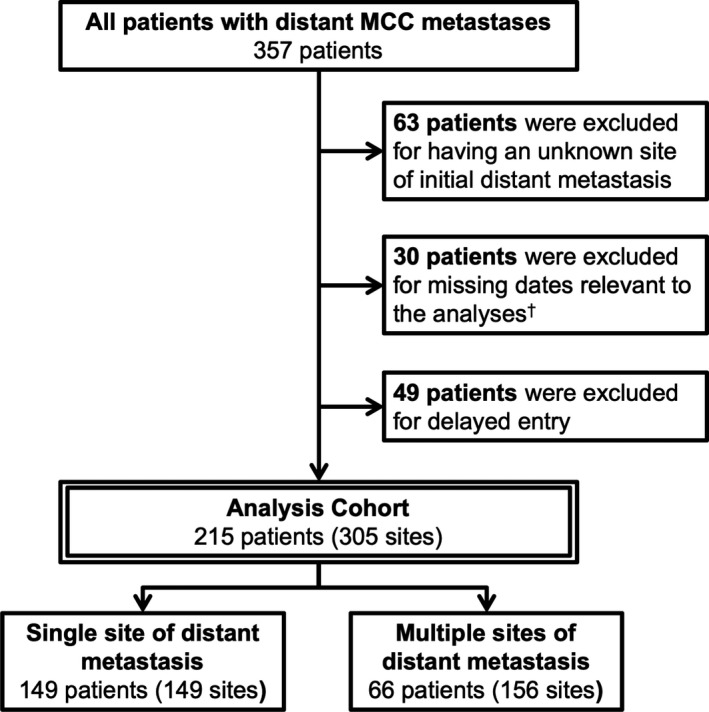
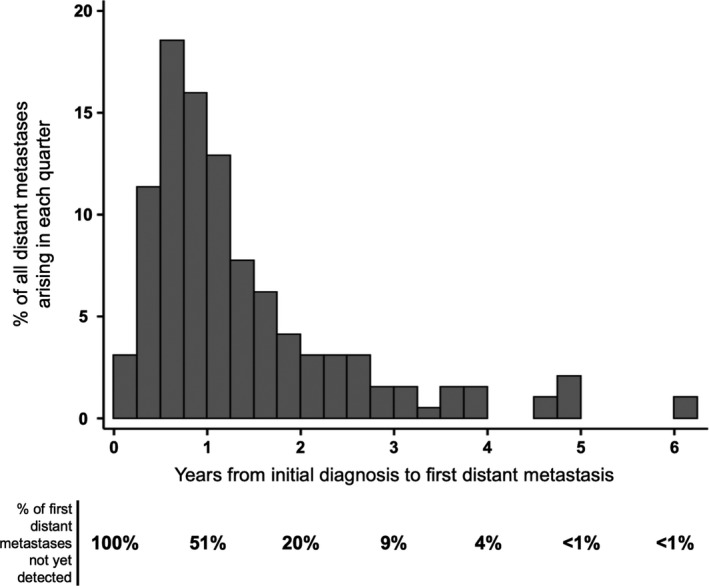
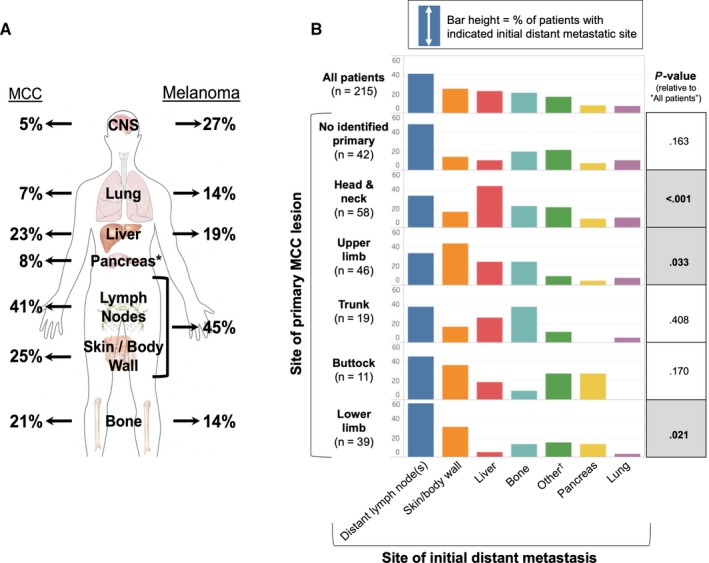
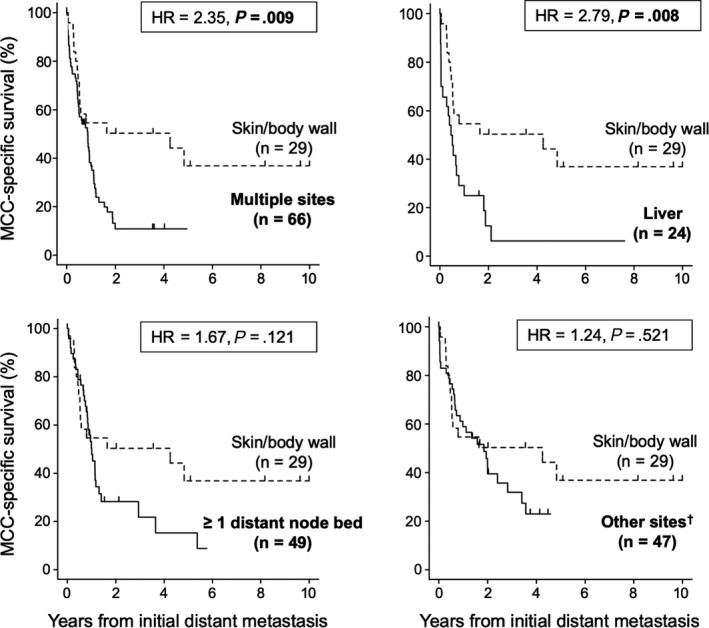
Approximately one-third of Merkel cell carcinoma (MCC) patients eventually develop distant metastatic disease. Little is known about whether the location of the primary lesion is predictive of initial distant metastatic site, or if survival likelihood differs depending on the metastatic site. Such data could inform imaging/surveillance practices and improve prognostic accuracy. Multivariate and competing-risk analyses were performed on a cohort of 215 MCC patients with distant metastases, 31% of whom had two or more initial sites of distant metastasis. At time of initial distant metastasis in the 215 patients, metastatic sites (n = 305) included non-regional lymph nodes (present in 41% of patients), skin/body wall (25%), liver (23%), bone (21%), pancreas (8%), lung (7%), and brain (5%). Among the 194 patients who presented with MCC limited to local or regional sites (stage I-III) but who ultimately developed distant metastases, distant progression occurred in 49% by 1 year and in 80% by 2 years following initial diagnosis. Primary MCC locations differed in how likely they were to metastasize to specific organs/sites (P < .001). For example, liver metastases were far more likely from a head/neck primary (43% of 58 patients) versus a lower limb primary (5% of 39 patients; P < .0001). Skin-only distant metastasis was associated with lower MCC-specific mortality as compared to metastases in multiple organs/sites (HR 2.7; P = .003), in the liver (HR 2.1; P = .05), or in distant lymph nodes (HR 2.0; P = .045). These data reflect outcomes before PD1-pathway inhibitor availability, which may positively impact survival. In conclusion, primary MCC location is associated with a pattern of distant spread, which may assist in optimizing surveillance. Because it is linked to survival, the site of initial distant metastasis should be considered when assessing prognosis.
Keywords: Merkel cell; carcinoma; dermatology; medical oncology; neoplasm metastasis; neoplasm staging; prognosis; radiology.
© 2019 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Chris Lewis received a grant from the American Cancer Society to perform this research. Kelly Paulson reports receiving research grants from SITC‐Merck, Bluebird Bioscience, and EMD‐Serono. Shailender Bhatia reports receiving grants from BMS, Merck, Novartis, EMD‐Serono, Oncosec, Immune Design, and NantKwest, as well as honoraria (for advisory board participation) from BMS, EMD‐Serono, and Sanofi‐Genzyme. Paul Nghiem reports receiving grant support from EMD Serono and Bristol Myers Squibb as well as honoraria from Merck and EMD‐Serono. Dan Hippe reported being a collaborator on industry‐funded work with GE Healthcare, Philips Healthcare, Toshiba America Medical Systems, and Siemens Medical Solutions USA. Ryan O'Malley reports receiving grant support from GE Healthcare. None of these disclosures were directly related to this publication.
Figures
References
-
- Albores‐Saavedra J, Batich K, Chable‐Montero F, Sagy N, Schwartz AM, Henson DE. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol. 2010;37(1):20‐27. - PubMed
-
- Paulson KG, Bhatia S. Advances in immunotherapy for metastatic Merkel cell carcinoma: a Clinician's Guide. J Natl Compr Canc Netw. 2018;16(6):782‐790. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
