

Complement fragments are biomarkers of antibody-mediated endothelial injury
- PMID: 31884386
- PMCID: PMC7192552
- DOI: 10.1016/j.molimm.2019.12.011
Complement fragments are biomarkers of antibody-mediated endothelial injury
Abstract
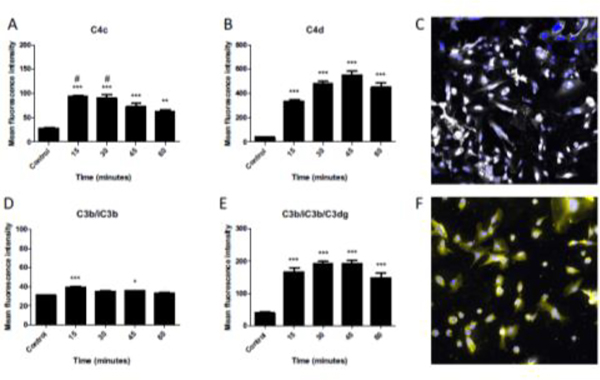
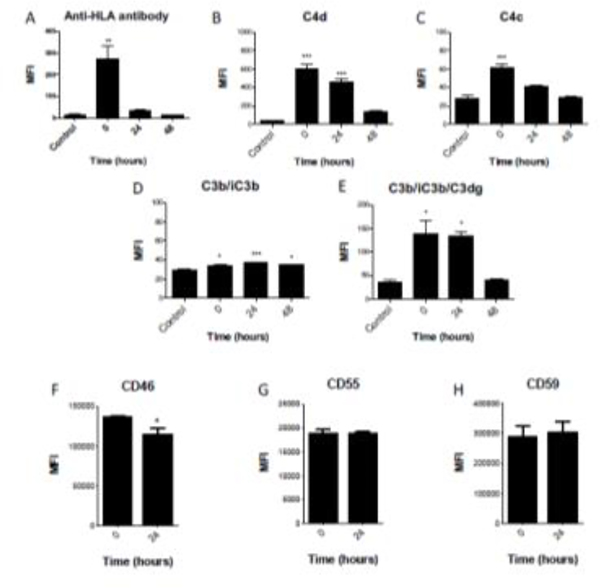
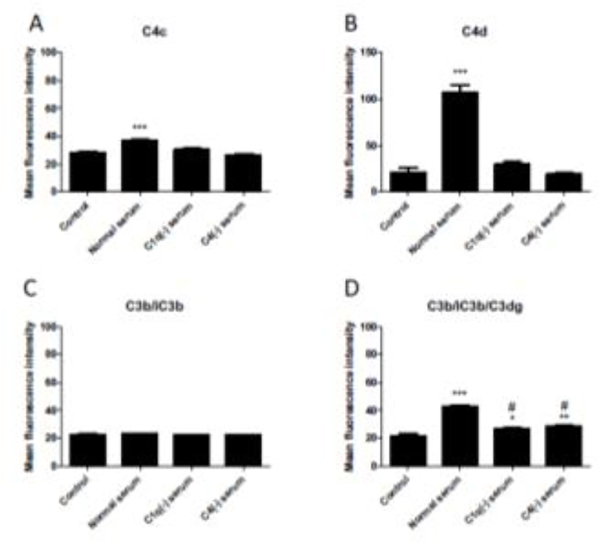
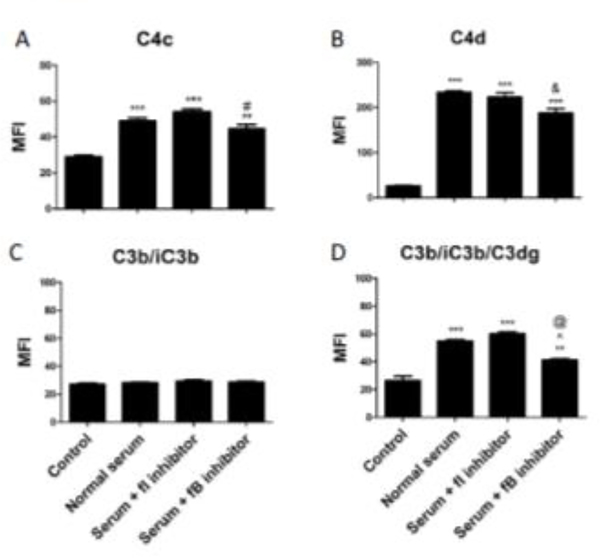
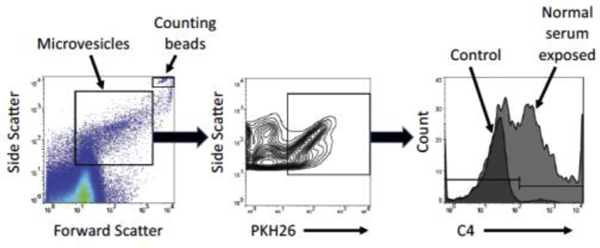
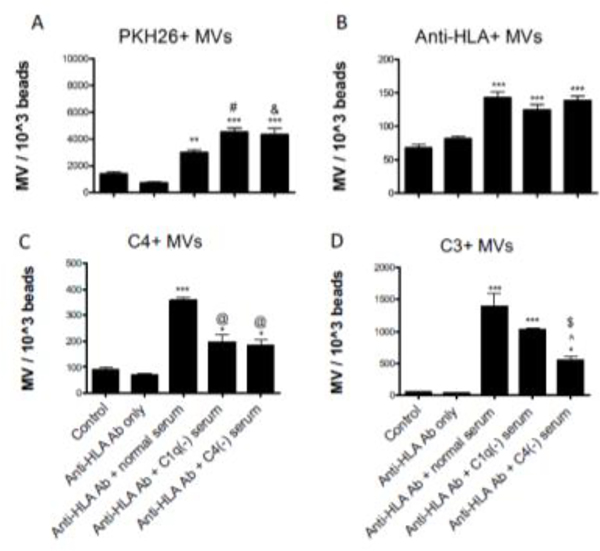
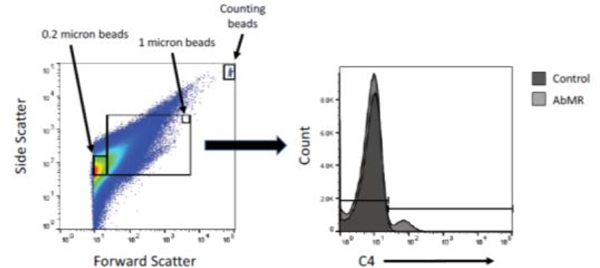
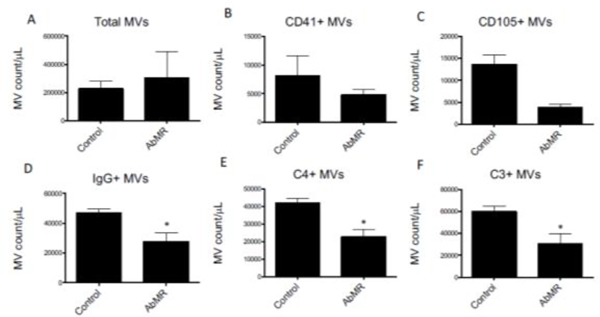
Antibody-mediated rejection (AbMR) adversely affects long-term graft survival in kidney transplantation. Currently, the diagnosis of AbMR requires a kidney biopsy, and detection of complement C4d deposition in the allograft is one of the diagnostic criteria. Complement activation also generates several soluble fragments which could potentially provide non-invasive biomarkers of the process. Furthermore, microvesicles released into the plasma from injured cells can serve as biomarkers of vascular injury. To explore whether soluble complement fragments or complement fragments bound to endothelial microvesicles can be used to non-invasively detect AbMR, we developed an in vitro model in which human endothelial cells were exposed to anti-HLA antibodies and complement sufficient serum. We found that complement fragments C4a and sC5b-9 were increased in the supernatants of cells exposed to complement-sufficient serum compared to cells treated complement-deficient serum. Furthermore, complement activation on the cell surface was associated with the release of microvesicles bearing C4 and C3 fragments. We next measured these analytes in plasma from kidney transplant recipients with biopsy-proven acute AbMR (n = 9) and compared the results with those from transplant recipients who also had impaired allograft function but who did not have AbMR (n = 30). Consistent with the in vitro results, complement fragments C4a and Ba were increased in plasma from patients with AbMR compared to control subjects (P < 0.001 and P < 0.01, respectively). Endothelial microvesicle counts were not increased in patients with AbMR, however, and the number of microvesicles with C4 and C3 bound to the surface was actually lower compared to control subjects (both P < 0.05). Our results suggest that plasma complement activation fragments may be useful as non-invasive biomarkers of antibody-mediated complement activation within the allograft. Complement-opsonized endothelial microvesicles are decreased in patients with AbMR, possibly due to enhanced clearance of microvesicles opsonized with C3 and C4 fragments.
Keywords: Antibody mediated rejection; Biomarker; Complement; Donor specific antibody.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures


References
-
- Anderson HC, Mulhall D, Garimella R, 2010. Role of extracellular membrane vesicles in the pathogenesis of various diseases, including cancer, renal diseases, atherosclerosis, and arthritis. Laboratory Investigation 90, 1549–1557. - PubMed
-
- Beyer C, Pisetsky DS, 2010. The role of microparticles in the pathogenesis of rheumatic diseases. Nature reviews. Rheumatology 6, 21–29. - PubMed
-
- Boulanger CM, Amabile N, Guerin AP, Pannier B, Leroyer AS, Mallat CN, Tedgui A, London GM, 2007. In vivo shear stress determines circulating levels of endothelial microparticles in end-stage renal disease. Hypertension 49, 902–908. - PubMed
-
- Chironi GN, Boulanger CM, Simon A, Dignat-George F, Freyssinet JM, Tedgui A, 2009. Endothelial microparticles in diseases. Cell Tissue Res 335, 143–151. - PubMed
-
- DiLillo DJ, Pawluczkowycz AW, Peng W, Kennedy AD, Beum PV, Lindorfer MA, Taylor RP, 2006. Selective and efficient inhibition of the alternative pathway of complement by a mAb that recognizes C3b/iC3b. Mol Immunol 43, 1010–1019. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
