

Multimodal Balance Training Supported by Rhythmical Auditory Stimuli in Parkinson's Disease: A Randomized Clinical Trial
- PMID: 31884492
- PMCID: PMC7029328
- DOI: 10.3233/JPD-191752
Multimodal Balance Training Supported by Rhythmical Auditory Stimuli in Parkinson's Disease: A Randomized Clinical Trial
Abstract
Background: Balance impairment in Parkinson's disease (PD) improves only partially with dopaminergic medication. Therefore, non-pharmacological interventions such as physiotherapy are important elements in clinical management. External cues are often applied to improve gait, but their effects on balance control are unclear.
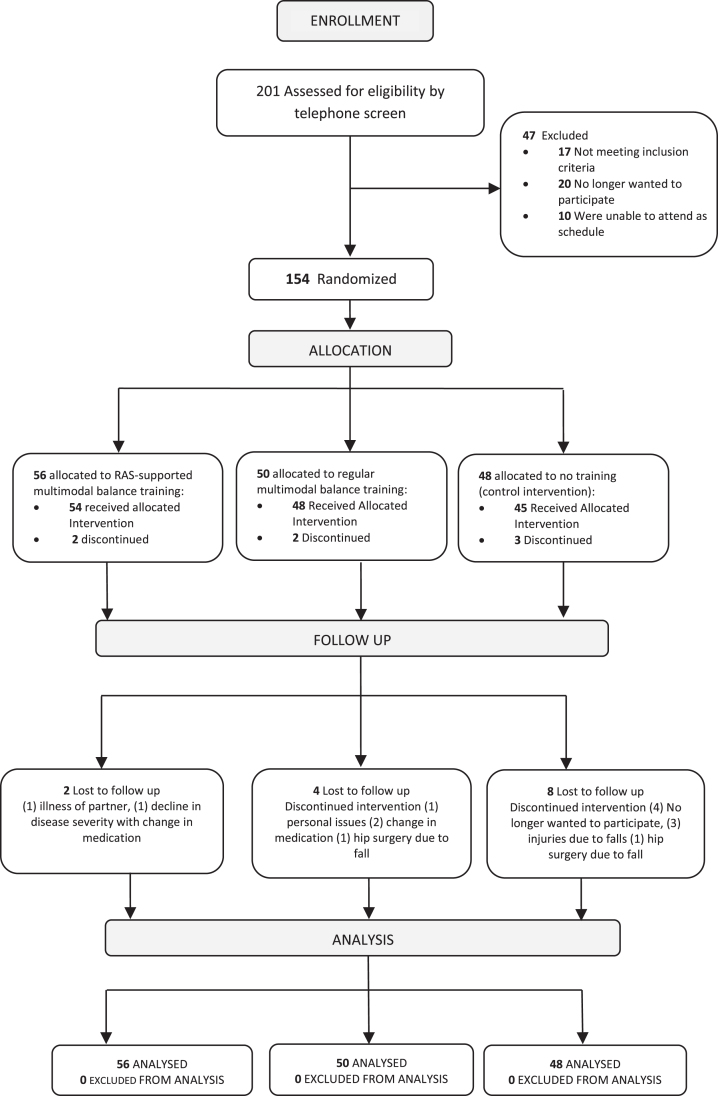
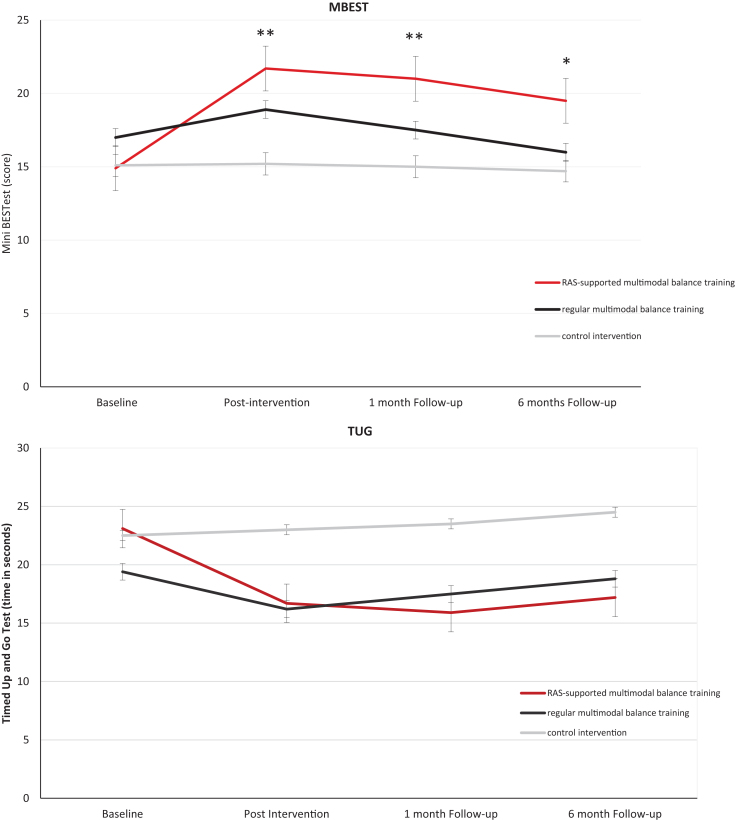
Objective/methods: We performed a prospective, single-blind, randomized clinical trial to study the effectiveness of balance training with and without rhythmical auditory cues. We screened 201 volunteers by telephone; 154 were assigned randomly into three groups: (1) multimodal balance training supported by rhythmical auditory stimuli (n = 56) (RAS-supported multimodal balance training); (2) regular multimodal balance training without rhythmical auditory stimuli (n = 50); and (3) control intervention involving a general education program (n = 48). Training was performed for 5 weeks, two times/week. Linear mixed models were used for all outcomes. Primary outcome was the Mini-BESTest (MBEST) score immediately after the training period. Assessments were performed by a single, blinded assessor at baseline, immediately post intervention, and after one and 6-months follow-up.
Results: Immediately post intervention, RAS-supported multimodal balance training was more effective than regular multimodal balance training on MBEST (difference 3.5 (95% Confidence Interval (CI) 2.2; 4.8)), p < 0.001). Patients allocated to both active interventions improved compared to controls (MBEST estimated mean difference versus controls 6.6 (CI 5.2; 8.0), p < 0.001 for RAS-supported multimodal balance training; and 3.0 (CI 2.7; 5.3), p < 0.001 for regular multimodal balance training). Improvements were retained at one-month follow-up for both active interventions, but only the RAS-supported multimodal balance training group maintained its improvement at 6 months.
Conclusion: Both RAS-supported multimodal balance training and regular multimodal balance training improve balance, but RAS-supported multimodal balance training-adding rhythmical auditory cues to regular multimodal balance training-has greater and more sustained effects.
Keywords: Parkinson’s disease; balance; clinical trial; cueing; physical therapy; postural control.
Conflict of interest statement
T.T.C. Capato, E.R. Barbosa, J. InHout, and J. Nonnekes: None; N.M. Vries. received a research grant by The Netherlands Organisation for Health Research and Development; B.R. Bloem received grant funding from the Netherlands Organization for Scientific Research, Michael J Fox Foundation, Parkinson Vereniging, Parkinson’s Foundation, Gatsby Foundation, Verily Life Sciences, Horizon 2020, Topsector Life Sciences and Health, Stichting Parkinson Fonds, AbbVie. Consultancy from Biogen, Abbvie, Walk with Path, UCB. Speaker fees from AbbVie, Zambon, Bial.
Figures
References
-
- Bloem BR, Hausdorff JM, Visser JE, Giladi N (2004) Falls and freezing of gait in Parkinson’s disease: A review of two interconnected, episodic phenomena. Mov Disord 19, 871–884. - PubMed
-
- Kalia LV, Lang AE (2015) Parkinson’s disease. Lancet 386, 896–912. - PubMed
-
- Ellis TD, Cavanaugh JT, Earhart GM, Ford MP, Foreman KB, Thackeray A, Thiese MS, Dibble LE (2016) Identifying clinical measures that most accurately reflect the progression of disability in Parkinson disease. Parkinsonism Relat Disord 25, 65–71. - PubMed
-
- van der Marck MA, Klok MP, Okun MS, Giladi N, Munneke M, Bloem BR (2014) Consensus-based clinical practice recommendations for the examination and management of falls in patients with Parkinson’s disease. Parkinsonism Relat Disord 20, 360–369. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
