

Eight-year post-trial follow-up of health care and long-term care costs of tele-based health coaching
- PMID: 31884682
- PMCID: PMC7080381
- DOI: 10.1111/1475-6773.13251
Eight-year post-trial follow-up of health care and long-term care costs of tele-based health coaching
Abstract
Objective: To evaluate the long-term effect of telephone health coaching on health care and long-term care (LTC) costs in type 2 diabetes (T2D) and coronary artery disease (CAD) patients.
Data sources/study setting: Randomized controlled trial (RCT) data were linked to Finnish national health and social care registries and electronic health records (EHR). Post-trial eight-year economic evaluation was conducted.
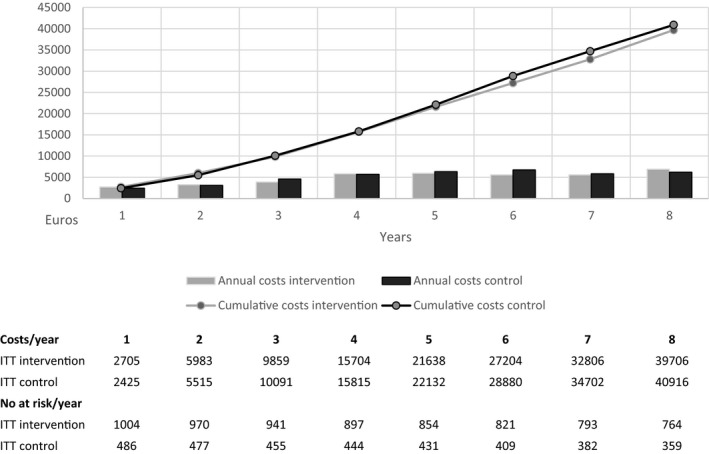
Study design: A total of 1,535 patients (≥45 years) were randomized to the intervention (n = 1034) and control groups (n = 501). The intervention group received monthly telephone health coaching for 12 months. Usual health care and LTC were provided for both groups.
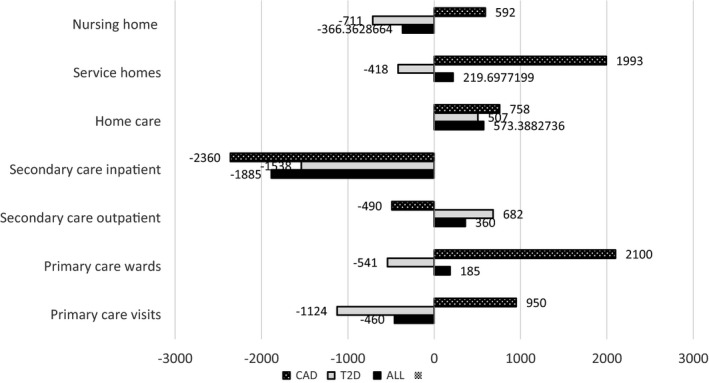
Principal findings: Intention-to-treat analysis showed no significant change in total health and long-term care costs (intervention effect €1248 [3 percent relative reduction], CI -6347 to 2217) in the intervention compared to the control group. There were also no significant changes among subgroups of patients with T2D or CAD.
Conclusions: Health coaching had a nonsignificant effect on health care and long-term care costs in the 8-year follow-up among patients with T2D or CAD. More research is needed to study, which patient groups, at which state of the disease trajectory of T2D and cardiovascular disease, would best benefit from health coaching.
Trial registration: ClinicalTrials.gov NCT00552903.
Keywords: coronary artery disease; costs; effectiveness; health coaching; type 2 diabetes.
© Health Research and Educational Trust.
Conflict of interest statement
None of the authors have any conflicts of interest to disclose.
Figures

References
-
- Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: Translating evidence into action. Health Affairs (Millwood). 2001;20(6):64‐78. - PubMed
-
- Mattke S, Seid M, Ma S. Evidence for the effect of disease management: Is $1 Billion a year a good investment? Am J Managed Care. 2007;13(12):670‐676. - PubMed
-
- Ellrodt G, Cook DJ, Lee J, et al. Evidence‐based disease management. JAMA. 1997;278(20):1687‐1692 - PubMed
-
- Hayes E, MacCahon C, Panahi MR, Hamre T, Pohlman K. Alliance not compliance: coaching strategies to improve type 2 diabetes outcomes. J Am Acad Nurse Pract. 2008;20:155‐162. - PubMed
-
- Palmer S, Tubbs I, Whybrow A. Health coaching to facilitate promotion of health behaviour and achievement of health‐related goals. Int J Health Promotion Educ. 2013;41:91‐93.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
