

Clinicopathological features of granulomatous lobular mastitis and mammary duct ectasia
- PMID: 31885718
- PMCID: PMC6924204
- DOI: 10.3892/ol.2019.11156
Clinicopathological features of granulomatous lobular mastitis and mammary duct ectasia
Abstract
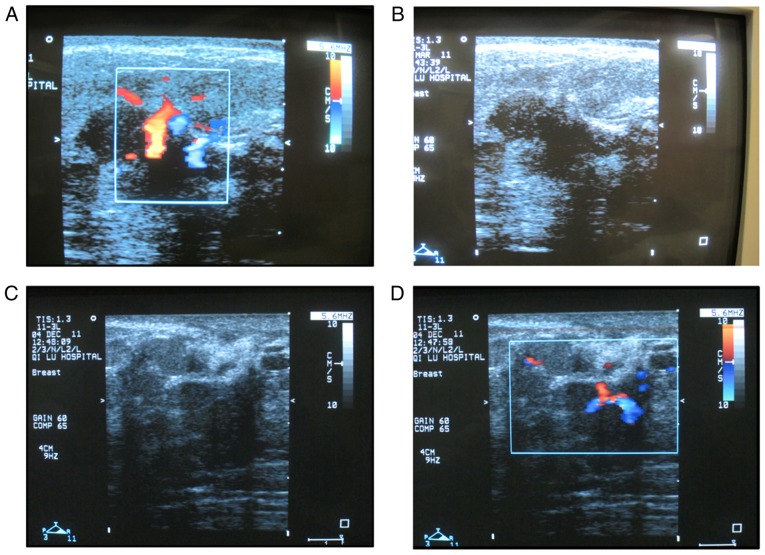
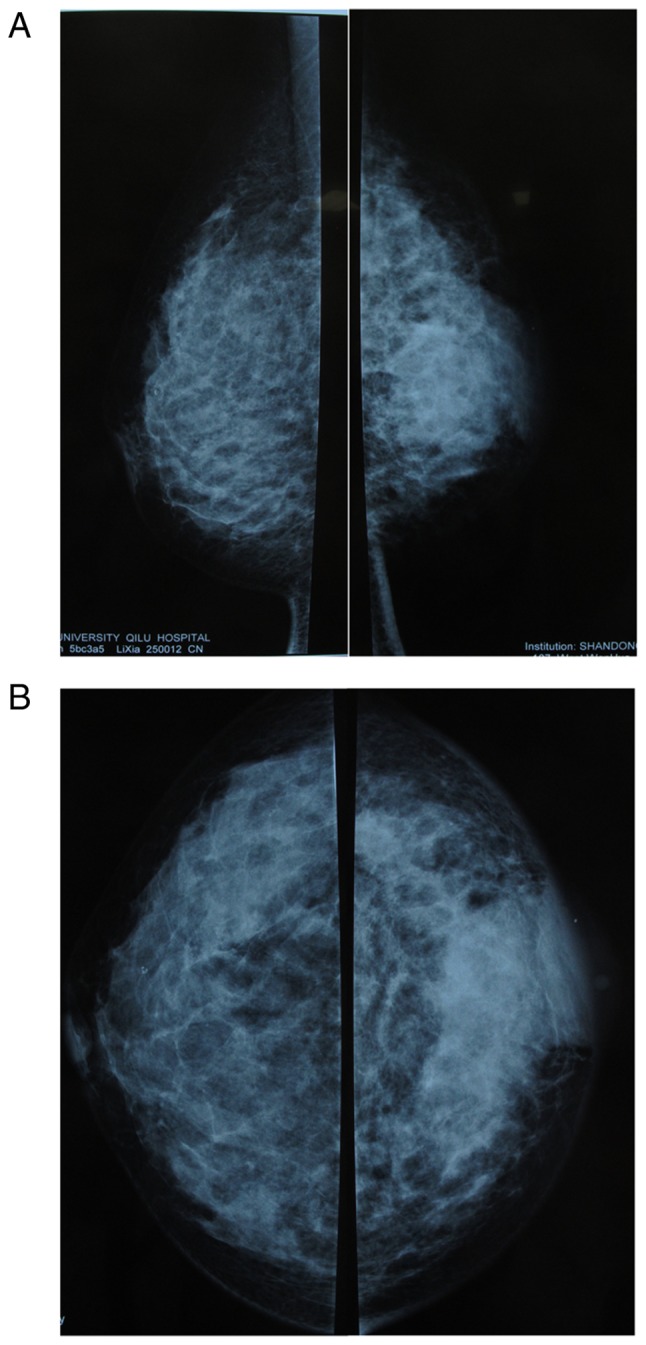
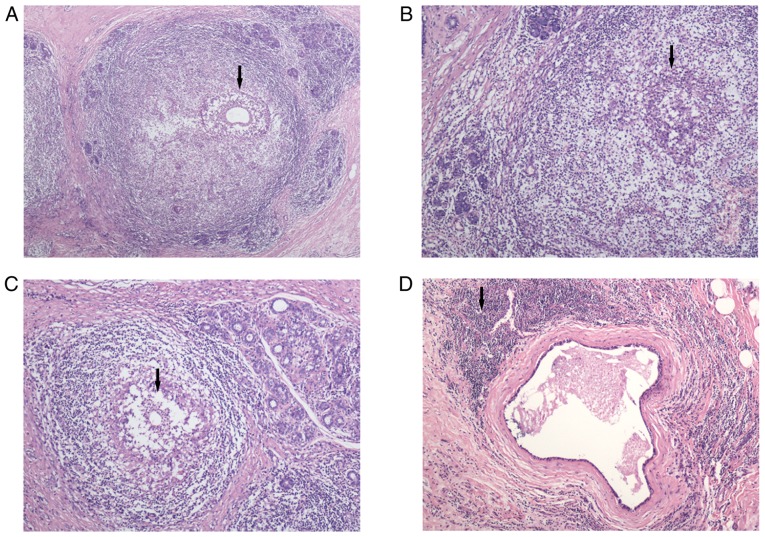
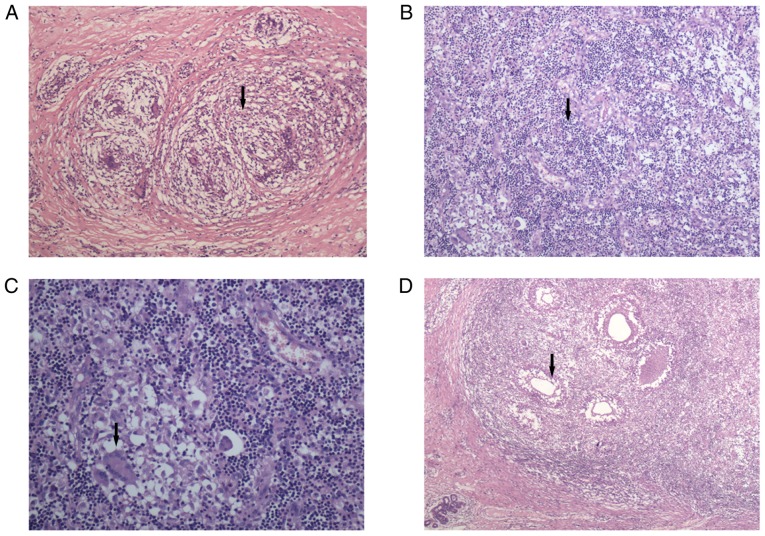
Granulomatous lobular mastitis (GLM) and mammary duct ectasia (MDE) are inflammatory diseases. However, only a limited number of studies have focused on characterizing their clinicopathological features. The aim of the present study was to investigate the etiology, clinicopathological characteristics and diagnosis of GLM and MDE. The clinical information and treatment of 118 female patients with pathologically-proven GLM or MDE were retrospectively analyzed in the present study. A total of 29 cases had GLM, 77 had MDE and 12 had GLM accompanied by MDE. GLM tends to occur in patients who have had their last birth within 5 years and are usually <40 years of age. GLM masses were usually larger than MDE masses and suppurated or ulcerated more easily. Histopathologically, GLM was characterized by a significant granulomatous inflammatory reaction centered on lobules. Compared with MDE, GLM had a higher incidence of granuloma and microabscess formation within the lobules and surrounding tissue. More multinucleated giant cells within granuloma were observed in patients with GLM than in those with MDE, while MDE was characterized by significant dilatation of the duct terminals and inflammatory changes in the duct wall and periductal tissues. When compared with patients with GLM, foam cells within the duct epithelium or surrounding stroma were more common in patients with MDE. The present study demonstrated that GLM and MDE had distinct clinicopathological characteristics. Further research is required in order to identify more appropriate treatment strategies for these specific types of breast inflammation.
Keywords: diagnosis; granulomatous lobular mastitis; mammary duct ectasia; pathology.
Copyright: © Jiang et al.
Figures

Similar articles
-
Identification of periductal mastitis and granulomatous lobular mastitis: a literature review.Ann Transl Med. 2023 Feb 15;11(3):158. doi: 10.21037/atm-22-6473. Epub 2023 Feb 3. Ann Transl Med. 2023. PMID: 36846004 Free PMC article. Review.
-
Periductal Mastitis, a Disease with Distinct Clinicopathological Features from Granulomatous Lobular Mastitis.J Inflamm Res. 2024 Jun 14;17:3815-3823. doi: 10.2147/JIR.S464585. eCollection 2024. J Inflamm Res. 2024. PMID: 38895142 Free PMC article.
-
Biomedical Indicators of Patients with Non-Puerperal Mastitis: A Retrospective Study.Nutrients. 2022 Nov 14;14(22):4816. doi: 10.3390/nu14224816. Nutrients. 2022. PMID: 36432503 Free PMC article.
-
Pathological manifestations of granulomatous lobular mastitis.Front Med (Lausanne). 2024 Feb 2;11:1326587. doi: 10.3389/fmed.2024.1326587. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38371511 Free PMC article. Review.
-
[Granulomatous lobular mastitis associated with mammary duct ectasia: a clinicopathologic study of 32 cases with review of literature].Zhonghua Bing Li Xue Za Zhi. 2013 Oct;42(10):665-8. Zhonghua Bing Li Xue Za Zhi. 2013. PMID: 24433728 Review. Chinese.
Cited by
-
Identification of periductal mastitis and granulomatous lobular mastitis: a literature review.Ann Transl Med. 2023 Feb 15;11(3):158. doi: 10.21037/atm-22-6473. Epub 2023 Feb 3. Ann Transl Med. 2023. PMID: 36846004 Free PMC article. Review.
-
The Effectiveness of Traditional Chinese Medicine Combined With Surgery to Treat Granulomatous Mastitis: A Propensity-Matched Analysis.Front Oncol. 2022 Feb 10;12:833742. doi: 10.3389/fonc.2022.833742. eCollection 2022. Front Oncol. 2022. PMID: 35223513 Free PMC article.
-
Differential expression profiles of miRNA in granulomatous lobular mastitis and identification of possible biomarkers.Exp Ther Med. 2022 Jun 8;24(2):500. doi: 10.3892/etm.2022.11427. eCollection 2022 Aug. Exp Ther Med. 2022. PMID: 35837043 Free PMC article.
-
Clinical therapeutic evaluation of vacuum sealing drainage and precise ultrasound-guided debridement in the treatment of non-lactational mastitis.Exp Ther Med. 2021 May;21(5):480. doi: 10.3892/etm.2021.9911. Epub 2021 Mar 12. Exp Ther Med. 2021. PMID: 33767775 Free PMC article.
-
Evaluation of the efficacy, prognosis and safety of dexamethasone in the treatment of different types of non-puerperal mastitis: A retrospective study.PLoS One. 2025 Jun 11;20(6):e0325739. doi: 10.1371/journal.pone.0325739. eCollection 2025. PLoS One. 2025. PMID: 40498798 Free PMC article.
References
LinkOut - more resources
Full Text Sources