

Immunotherapy- (Blinatumomab-) Related Lineage Switch of KMT2A/AFF1 Rearranged B-Lymphoblastic Leukemia into Acute Myeloid Leukemia/Myeloid Sarcoma and Subsequently into B/Myeloid Mixed Phenotype Acute Leukemia
- PMID: 31885955
- PMCID: PMC6925828
- DOI: 10.1155/2019/7394619
Immunotherapy- (Blinatumomab-) Related Lineage Switch of KMT2A/AFF1 Rearranged B-Lymphoblastic Leukemia into Acute Myeloid Leukemia/Myeloid Sarcoma and Subsequently into B/Myeloid Mixed Phenotype Acute Leukemia
Abstract
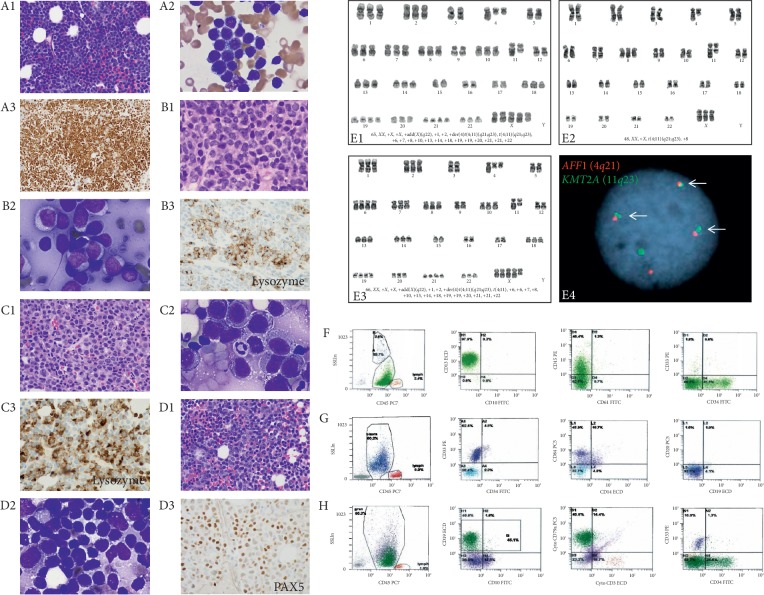
The presence of KMT2A/AFF1 rearrangement in B-lymphoblastic leukemia (B-ALL) is an independent poor prognostic factor and has been associated with higher rate of treatment failure and higher risk of linage switch under therapy. Blinatumomab has shown promising therapeutic results in refractory or relapsed B-ALL; however, it has potential risk of inducing lineage switch, especially in KMT2A/AFF1 rearranged B-ALL into acute myeloid leukemia and/or myeloid sarcoma. We report a 40-year-old female with KMT2A/AFF1-rearranged B-ALL that was refractory to conventional chemotherapy. Following administration of blinatumomab, she developed a breast mass proven to be myeloid sarcoma, in addition to bone marrow involvement by AML. Approximately six weeks after cessation of blinatumomab, a repeat bone marrow examination revealed B/myeloid MPAL.
Copyright © 2019 Rui R. He et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Wölfl M., Rasche M., Eyrich M., Schmid R., Reinhardt D., Schlegel P. G. Spontaneous reversion of a lineage switch following an initial blinatumomab-induced ALL-to-AML switch in MLL-rearranged infant ALL. Blood Advances. 2018;2(12):1382–1385. doi: 10.1182/bloodadvances.2018018093. - DOI - PMC - PubMed
-
- Fournier E., Inchiappa L., Delattre C., et al. Increased risk of adverse acute myeloid leukemia after anti-CD19-targeted immunotherapies in KMT2A-rearranged acute lymphoblastic leukemia: a case report and review of the literature. Leukemia and Lymphoma. 2019;60(7):1827–1830. doi: 10.1080/10428194.2018.1562185. - DOI - PubMed
-
- Haddox C. L., Mangaonkar A. A., Chen D., et al. Blinatumomab-induced lineage switch of B-ALL with t(4:11)(q21;q23) KMT2A/AFF1 into an aggressive AML: pre- and post-switch phenotypic, cytogenetic and molecular analysis. Blood Cancer Journal. 2017;7(9):p. e607. doi: 10.1038/bcj.2017.89. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
