

Asymptomatic Cardiac Metastases From Esophageal Cancer: A Case Report Of Ante-mortem Detection And Literature Review
- PMID: 31886099
- PMCID: PMC6913947
- DOI: 10.7759/cureus.6387
Asymptomatic Cardiac Metastases From Esophageal Cancer: A Case Report Of Ante-mortem Detection And Literature Review
Abstract
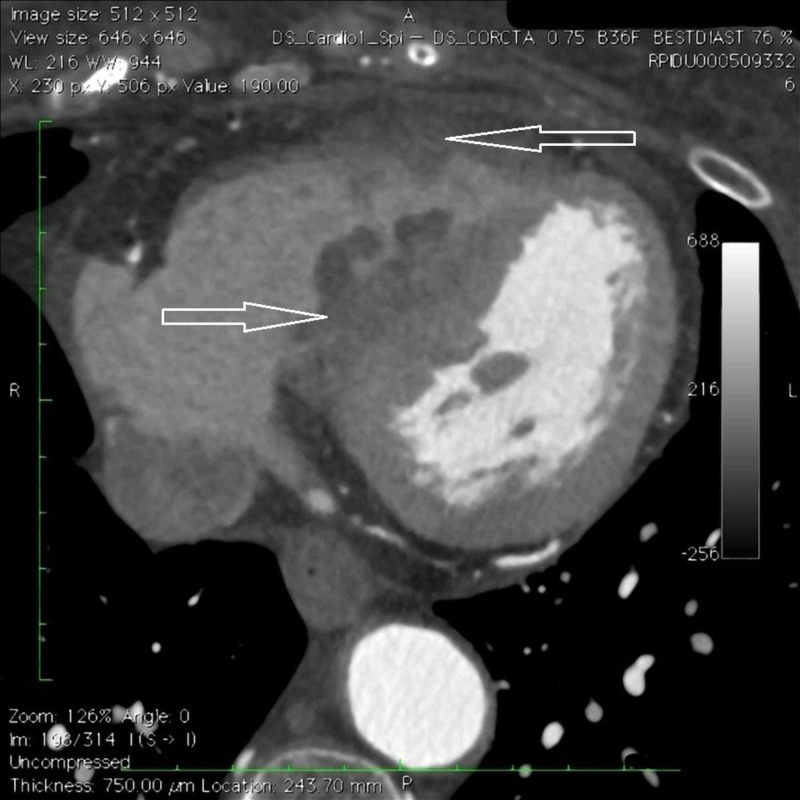
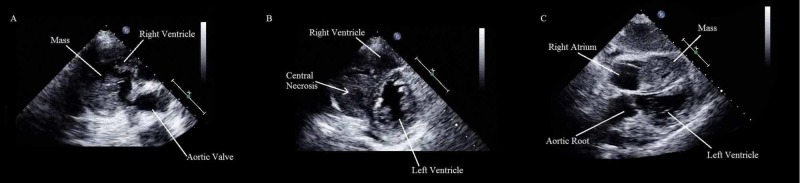
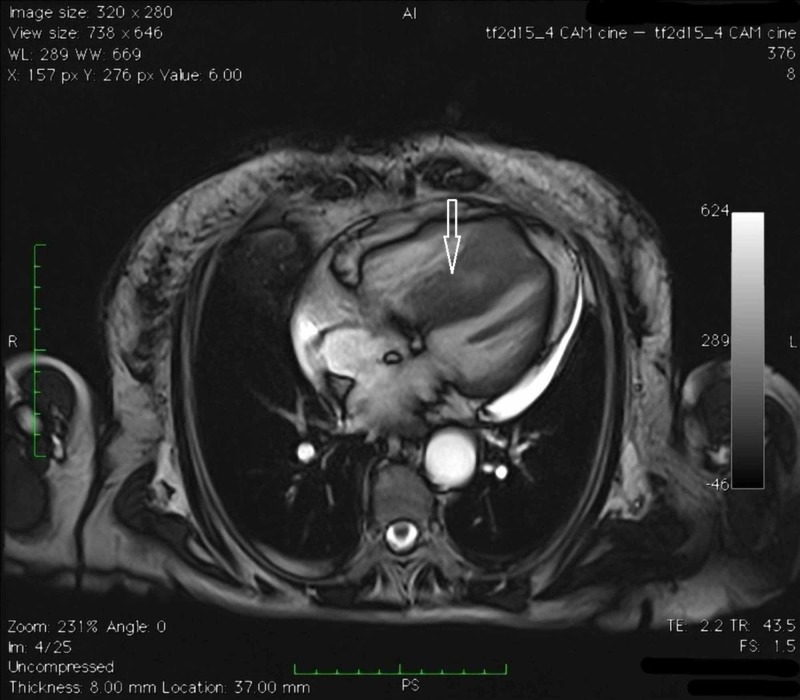
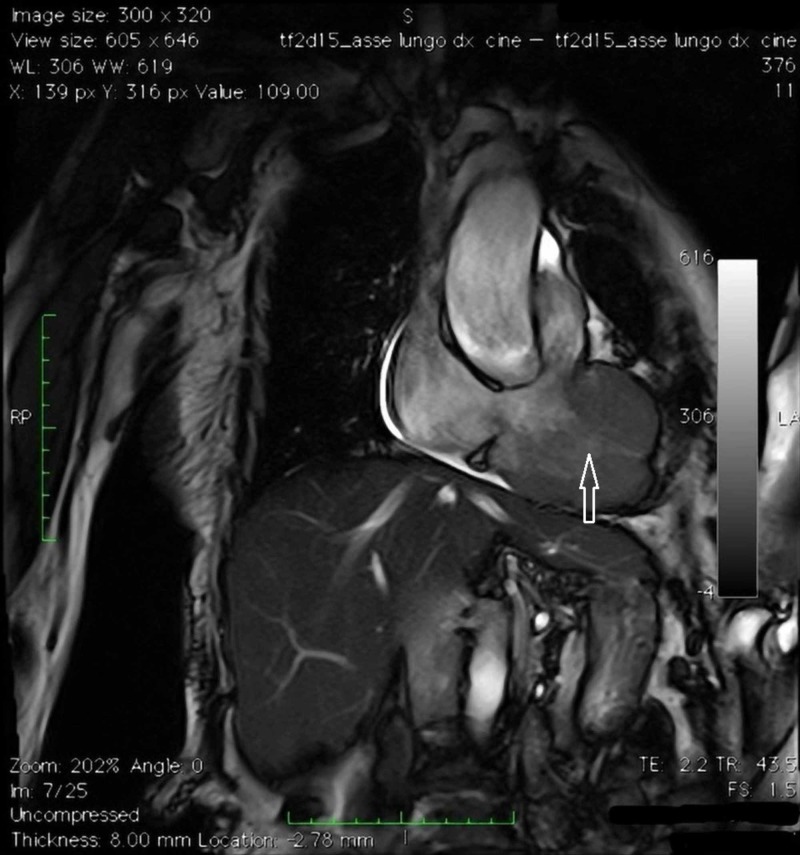
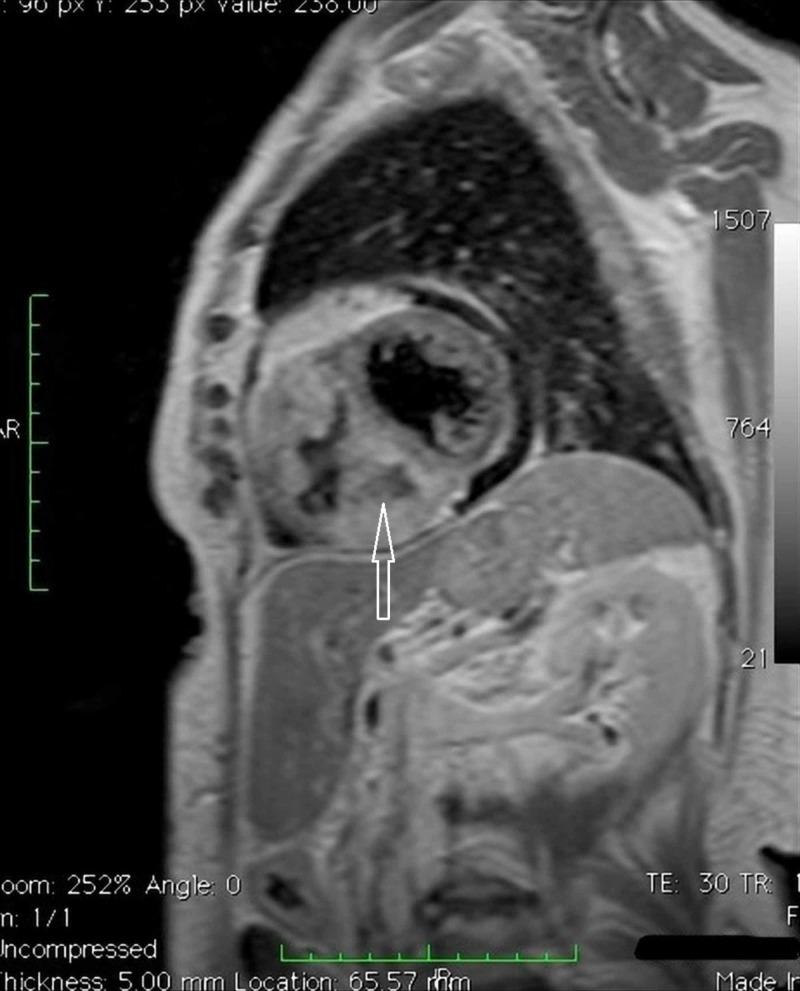
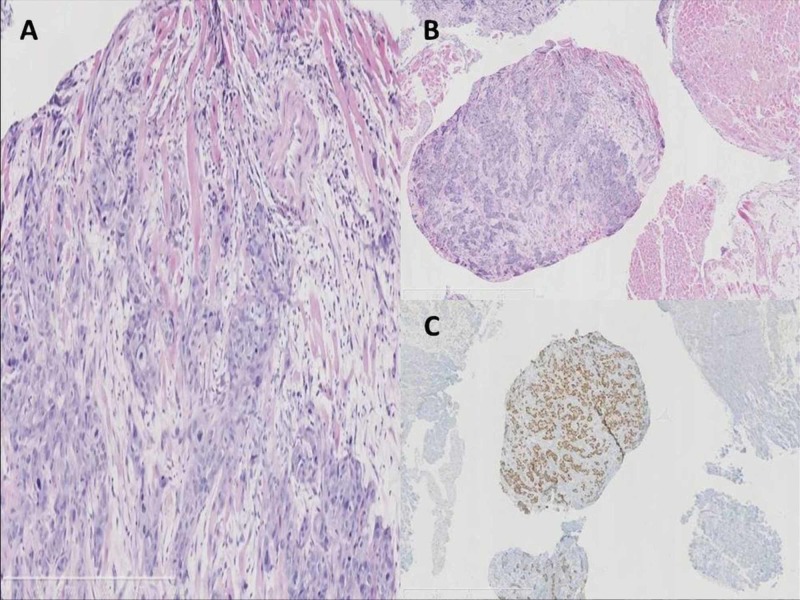
Metastatic spread to the heart from neoplasms is very rare, often silent and rarely gains clinical attention. Usually, it correlates with widespread metastatic disease and is suggestive of a poor prognosis. Most cardiac metastases (CM) are detected following post-mortem studies with only a handful reported antemortemly. Here, we report a case of an asymptomatic cardiac metastasis from esophageal carcinoma and a review of the literature. In late July 2014, a 73-year-old woman diagnosed with locally advanced esophageal squamous cell carcinoma was admitted to our institution. Cardiothoracic metastases were not detected at basal computed tomography (CT) scan. The patient was submitted to concurrent cisplatin and radiotherapy. Just before surgery, a CT scan revealed two metastases in the right ventricle and in the interventricular septum. Transthoracic echocardiography and an endomyocardial biopsy confirmed the diagnosis of squamous cell carcinoma from the esophageal origin. In February 2015, chemotherapy was started, but after two courses of gemcitabine, a pulmonary embolism and then a congestive heart failure caused death of the patient on April 2015. Reviewing the literature, 14 cases with an antemortem diagnosis of CM from esophageal cancer were reported. Our patient should be the fifteenth case with an uncommon presentation without symptoms or signs in the diagnosis. Our case highlights that patients should be evaluated using echocardiography for CM, even if asymptomatic.
Keywords: ante-mortem detection; cancer case report; cardiac imaging; cardiac metastases; esophageal cancer.
Copyright © 2019, Signorelli et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Secondary cardiac tumor originating from laryngeal carcinoma: case report and review of the literature. Renders F, Vanderhyden M, Andries E. Acta Cardiol. 2005;60:57–60. - PubMed
-
- A 30-year analysis of cardiac neoplasms at autopsy. Butany J, Leong SW, Carmichael K, Komeda M. https://www.ncbi.nlm.nih.gov/pubmed/16003450. Can J Cardiol. 2005;21:675–680. - PubMed
-
- Sudden death from metastatic esophageal cancer to the ventricular septum. Kataoka M, Shigemitsu K, Tanabe S, Ohara T, Takahata T, Nose S. Jpn J Thorac Cardiovasc Surg. 2005;53:365–368. - PubMed
-
- Oesophageal cancer with myocardial metastasis complicated by ventricular fibrillation: the role of echocardiography. Karabay CY, Kocabay G, Toprak C, Kirma C. https://www.ncbi.nlm.nih.gov/pubmed/22430418. Kardiol Pol. 2012;70:296–297. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous