

Longitudinal assessments highlight long-term behavioural recovery in disorders of consciousness
- PMID: 31886461
- PMCID: PMC6924536
- DOI: 10.1093/braincomms/fcz017
Longitudinal assessments highlight long-term behavioural recovery in disorders of consciousness
Abstract
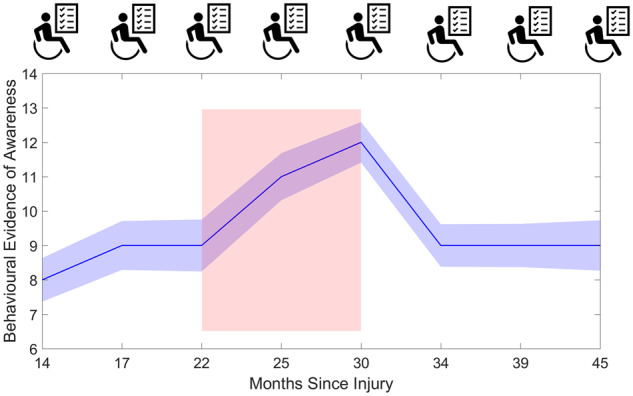
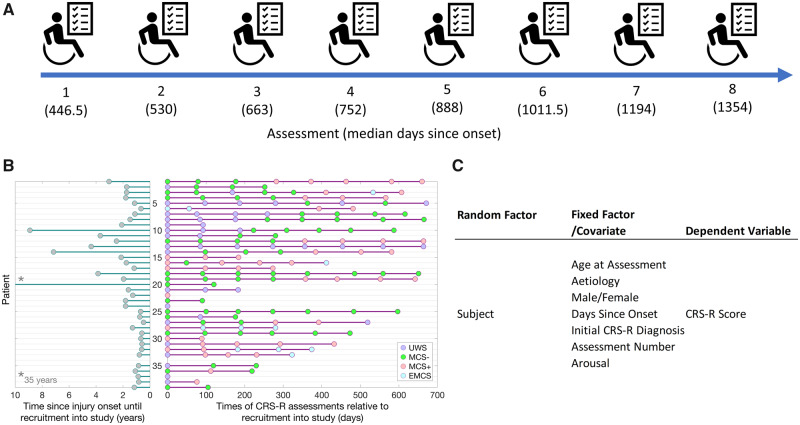
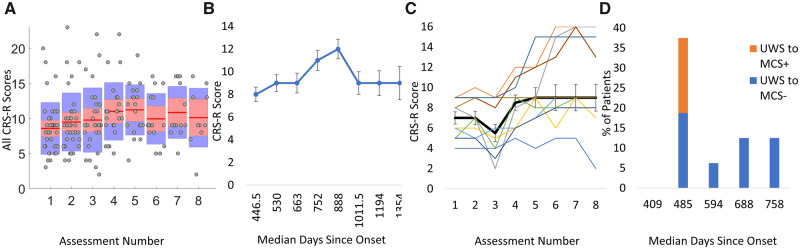
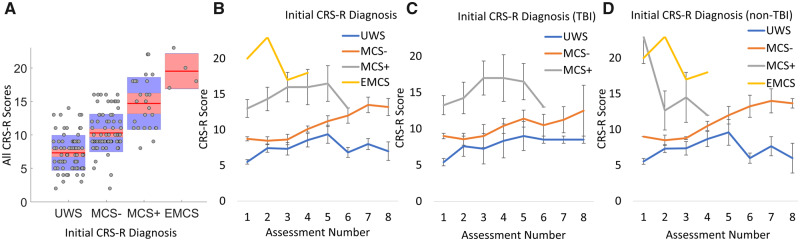
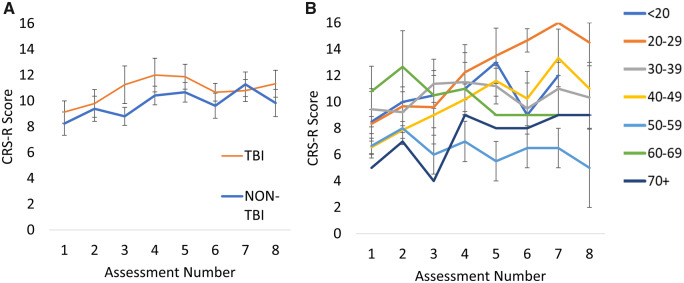
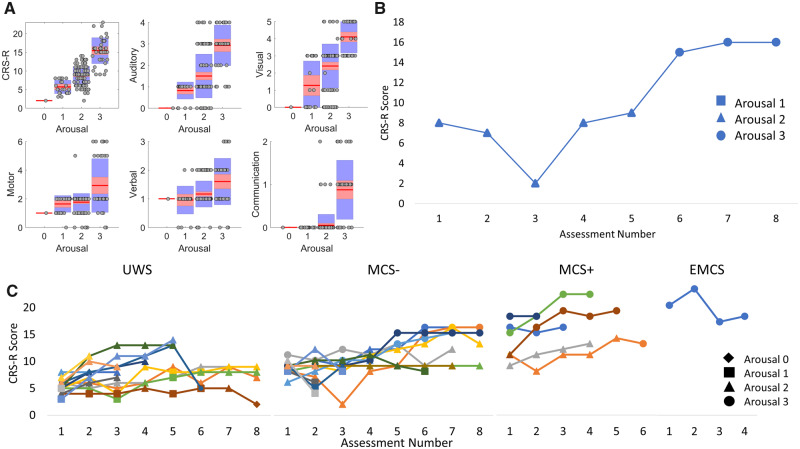
Accurate diagnosis and prognosis of disorders of consciousness is complicated by the variability amongst patients' trajectories. However, the majority of research and scientific knowledge in this field is based on cross-sectional studies. The translational gap in applying this knowledge to inform clinical management can only be bridged by research that systematically examines follow-up. In this study, we present findings from a novel longitudinal study of the long-term recovery trajectory of 39 patients, repeatedly assessed using the Coma Recovery Scale-Revised once every 3 months for 2 years, generating 185 assessments. Despite the expected inter-patient variability, there was a statistically significant improvement in behaviour over time. Further, improvements began approximately 22 months after injury. Individual variation in the trajectory of recovery was influenced by initial diagnosis. Patients with an initial diagnosis of unresponsive wakefulness state, who progressed to the minimally conscious state, did so at a median of 485 days following onset-later than 12-month period after which current guidelines propose permanence. Although current guidelines are based on the expectation that patients with traumatic brain injury show potential for recovery over longer periods than those with non-traumatic injury, we did not observe any differences between trajectories in these two subgroups. However, age was a significant predictor, with younger patients showing more promising recovery. Also, progressive increases in arousal contributed exponentially to improvements in behavioural awareness, especially in minimally conscious patients. These findings highlight the importance of indexing arousal when measuring awareness, and the potential for interventions to regulate arousal to aid long-term behavioural recovery in disorders of consciousness.
Keywords: Coma Recovery Scale-Revised; arousal; disorders of consciousness; longitudinal; natural history.
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Bagnato S, Boccagni C, Sant'Angelo A, Fingelkurts AA, Fingelkurts AA, Galardi G.. Longitudinal assessment of clinical signs of recovery in patients with unresponsive wakefulness syndrome after traumatic or nontraumatic brain injury. J Neurotrauma 2017; 34: 535–9. - PubMed
-
- Braakman R, Jennett W, Minderhoud J.. Prognosis of the posttraumatic vegetative state. Acta Neurochir 1988; 95: 49–52. - PubMed
-
- Candelieri A, Cortese MD, Dolce G, Riganello F, Sannita WG.. Visual pursuit: within-day variability in the severe disorder of consciousness. J Neurotrauma 2011; 28: 2013–7. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous