

Preoperative Ascorbic Acid Levels in Proximal Femur Fracture Patients Have No Postoperative Clinical Impact, While Ascorbic Acid Levels upon Discharge Have a Major Effect on Postoperative Outcome
- PMID: 31888071
- PMCID: PMC7019571
- DOI: 10.3390/jcm9010066
Preoperative Ascorbic Acid Levels in Proximal Femur Fracture Patients Have No Postoperative Clinical Impact, While Ascorbic Acid Levels upon Discharge Have a Major Effect on Postoperative Outcome
Abstract
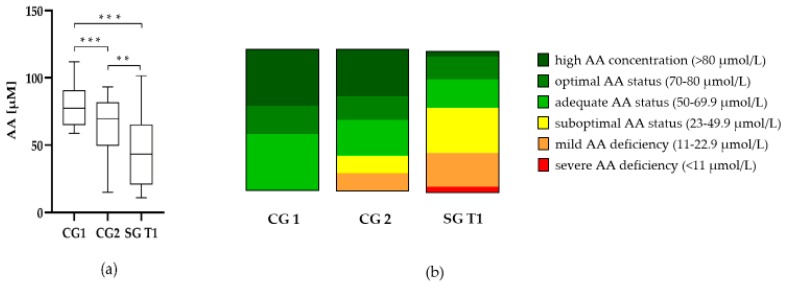
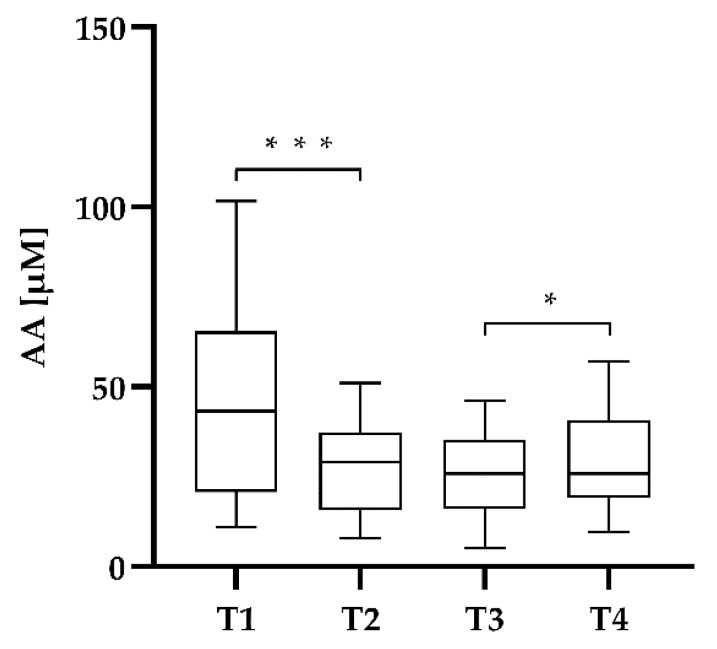
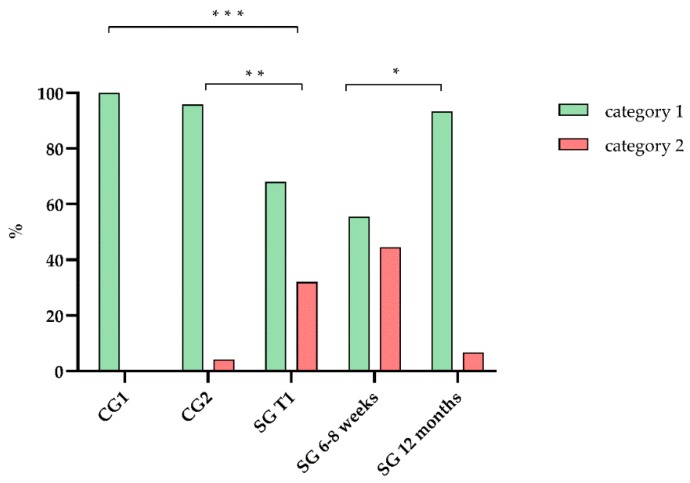
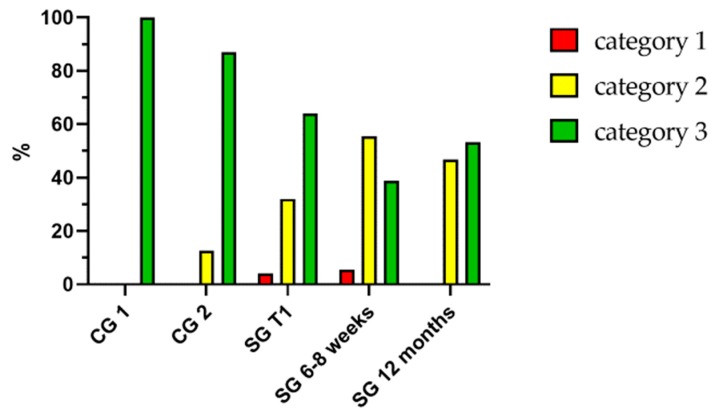
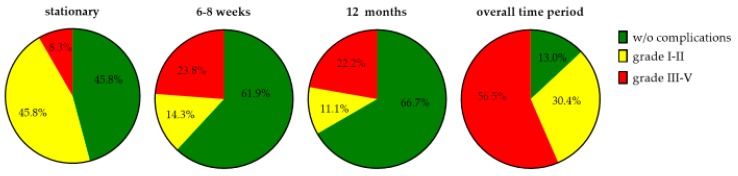
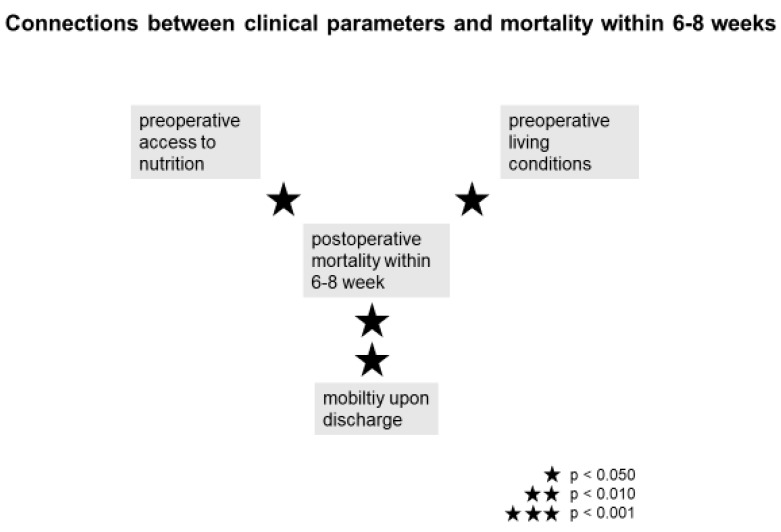
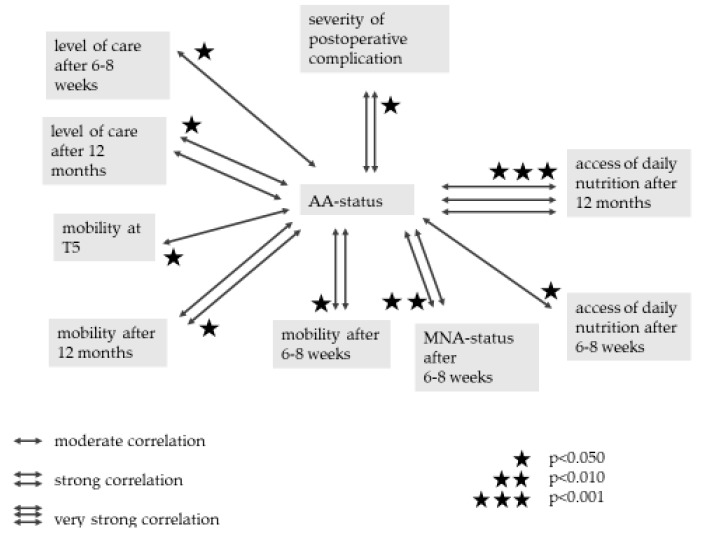
Proximal femur fractures show a high prevalence in elderly patients and are associated with an elevated risk of multimorbidity and early mortality. Recovery is impaired by malnutrition and oxidative stress, which is affected by antioxidants such as ascorbic acid (AA). This study monitored AA levels during hospitalization of patients with a proximal femur to investigate the influence of AA status to the clinical outcome. AA levels of 25 elderly patients with a proximal femur fracture were measured during hospitalization using high performance liquid chromatography. Plasma samples were collected preoperatively, on the first day after surgery, on the third day after surgery and on the day of discharge. Nutritional Risk Screening 2002 (NRS) and Mini Nutritional Assessment (MNA) were assessed to evaluate the nutritional status. In patients with proximal femoral fractures, preoperative AA concentrations were significantly lower compared to elderly patients without an acute fracture. A significant decrease of 33.8% in AA plasma level was measured on the day after surgery with a significant recovery up to the time of discharge. The preoperative AA status did not have any significant effect on clinical outcome. However, inadequate AA levels (<50 µmol/L) upon discharge significantly increased the incidence and the severity of postoperative complications. These results indicate that the AA status upon discharge has a greater impact on clinical outcome than assumed, and therefore, AA supplementation during hospitalization should be considered.
Keywords: MNA; NRS; ascorbic acid; geriatric patients; malnutrition; oxidative stress; proximal femoral fracture; reactive oxygen species.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ihle C., Freude T., Bahrs C., Zehendner E., Braunsberger J., Biesalski H.K., Lambert C., Stockle U., Wintermeyer E., Grunwald J., et al. Malnutrition—An underestimated factor in the inpatient treatment of traumatology and orthopedic patients: A prospective evaluation of 1055 patients. Injury. 2017;48:628–636. doi: 10.1016/j.injury.2017.01.036. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
