

The Diagnosis and Treatment of Hypertriglyceridemia
- PMID: 31888796
- PMCID: PMC6962767
- DOI: 10.3238/arztebl.2019.0825
The Diagnosis and Treatment of Hypertriglyceridemia
Abstract
Background: Hypertriglyceridemia affects 15-20% of the adult population and is associated with overweight, metabolic syndrome, and diabetes mellitus. It is often discovered incidentally.
Methods: This review is based on pertinent publications retrieved by a selective literature search, including current guidelines on hypertriglyceridemia.
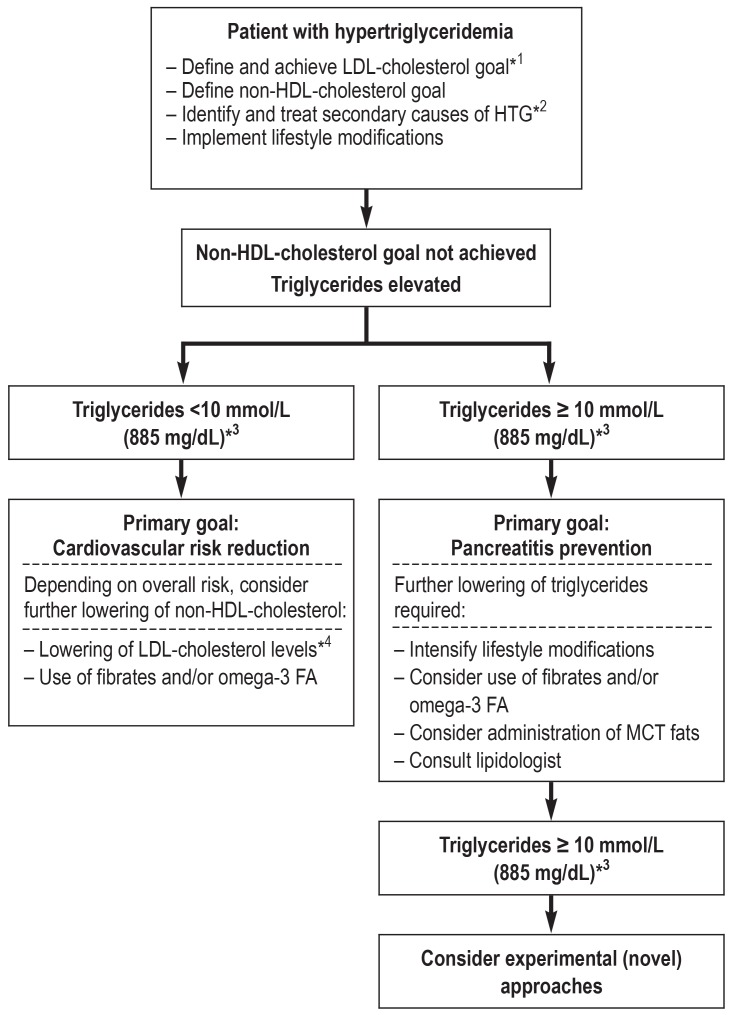
Results: Elevated triglyceride (TG) levels are causally linked to cardiovascular disease; TG levels above 1000 mg/dL (11.4 mmol/L) can induce acute pancreatitis. The individual risk of cardiovascular disease and of pancreatitis must be estimated in order to decide whether, and how, hypertriglyceridemia should be treated. Lifestyle modifications (cessation of alcohol consumption, reduced intake of rapidly metabolized carbohydrates), weight loss, and blood sugar control are the most effective ways to lower TG levels. The need to lower the low-density lipoprotein (LDL) concentration must be determined on the basis of the cardiovascular risk, independently of the success of the lifestyle changes. Few patients need specific drug treatment to lower the TG level. Fibrates can lower TG concentrations, but their efficacy in combination with statins has not been clearly shown in endpoint studies. A daily dose of 2-4 g omega-3 fatty acids can also lower TG levels. To date, only a single large-scale randomized, blinded trial has shown the efficacy of 4 g of eicosapentaenoic acid ethyl ester per day in lowering the risk in high-risk patients (number needed to treat = 21). Patients with the very rare purely genetic types of hypertriglyceridemia (familial chylomicronemia syndrome) should be treated in specialized outpatient clinics.
Conclusion: Hypertriglyceridemia is causally linked to cardiovascular disease and pancreatitis. Lifestyle modifications play a paramount role in its treatment.
Figures
Comment in
-
Measuring Triglycerides Is Mostly not Necessary.Dtsch Arztebl Int. 2020 Mar 27;117(13):224. doi: 10.3238/arztebl.2020.0224a. Dtsch Arztebl Int. 2020. PMID: 32343666 Free PMC article. No abstract available.
References
-
- Jaross W, Assmann G, Bergmann S, et al. Comparison of risk factors for coronary heart disease in Dresden and Munster. Results of the DRECAN (Dresden Cardiovascular Risk and Nutrition) study and the PROCAM (Prospective Cardiovascular Munster) Study. Eur J Epidemiol. 1994;10:307–315. - PubMed
-
- Arca M, Borghi C, Pontremoli R, et al. Hypertriglyceridemia and omega-3 fatty acids: Their often overlooked role in cardiovascular disease prevention. Nutr Metab Cardiovasc Dis. 2018;28:197–205. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines Circulation. J Am Coll Cardiol. 2019;73:3168–3209. - PubMed
-
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2019 doi: 10.1093/eurheartj/ehz455. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous