

Average medical cost of fatal and non-fatal injuries by type in the USA
- PMID: 31888976
- PMCID: PMC7326639
- DOI: 10.1136/injuryprev-2019-043544
Average medical cost of fatal and non-fatal injuries by type in the USA
Erratum in
-
Correction: Average medical cost of fatal and non-fatal injuries by type in the USA.Inj Prev. 2021 Oct;27(5):506. doi: 10.1136/injuryprev-2019-043544corr1. Epub 2021 Jul 27. Inj Prev. 2021. PMID: 34315828 No abstract available.
Abstract
Objective: To estimate the average medical care cost of fatal and non-fatal injuries in the USA comprehensively by injury type.
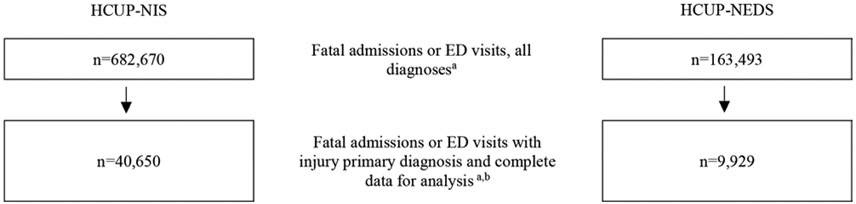
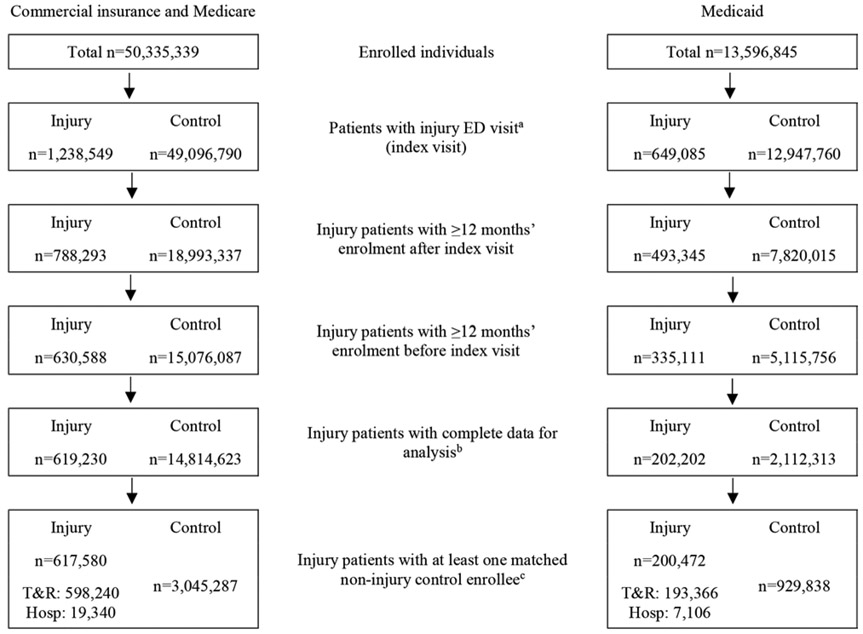
Methods: The attributable cost of injuries was estimated by mechanism (eg, fall), intent (eg, unintentional), body region (eg, head and neck) and nature of injury (eg, fracture) among patients injured from 1 October 2014 to 30 September 2015. The cost of fatal injuries was the multivariable regression-adjusted average among patients who died in hospital emergency departments (EDs) or inpatient settings as reported in the Healthcare Cost and Utilization Project Nationwide Emergency Department Sample and National Inpatient Sample, controlling for demographic (eg, age), clinical (eg, comorbidities) and health insurance (eg, Medicaid) factors. The 1-year attributable cost of non-fatal injuries was assessed among patients with ED-treated injuries using MarketScan medical claims data. Multivariable regression models compared total medical payments (inpatient, outpatient, drugs) among non-fatal injury patients versus matched controls during the year following injury patients' ED visit, controlling for demographic, clinical and insurance factors. All costs are 2015 US dollars.
Results: The average medical cost of all fatal injuries was approximately $6880 and $41 570 per ED-based and hospital-based patient, respectively (range by injury type: $4764-$10 289 and $31 912-$95 295). The average attributable 1-year cost of all non-fatal injuries per person initially treated in an ED was approximately $6620 (range by injury type: $1698-$80 172).
Conclusions and relevance: Injuries are costly and preventable. Accurate estimates of attributable medical care costs are important to monitor the economic burden of injuries and help to prioritise cost-effective public health prevention activities.
Keywords: barell matrix; costs; mechanism.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Murphy SL, Xu J, Kochanek KD, et al. Mortality in the United States, 2017. NCHS Data Brief 2018:1–8. - PubMed
-
- National Center for Injury Prevention and Control. Web-Based injury statistics query and reporting system (WISQARS). Atlanta, GA: Centers for Disease Control and Prevention, 2019. https://www.cdc.gov/injury/wisqars/nonfatal.html
-
- US Bureau of Economic Analysis. Health care satellite account: blended account, 2000–2016 Suidland, MD, 2018. Available: https://www.bea.gov/data/special-topics/health-care
-
- Lawrence B, Miller T. Medical and work loss cost estimation methods for the WISQARS cost of injury module. Calverton, MD: Pacific Institute for Research & Evaluation, 2010.
-
- Florence C, Haegerich T, Simon T, et al. Estimated Lifetime Medical and Work-Loss Costs of Emergency Department-Treated Nonfatal Injuries--United States, 2013. MMWR Morb Mortal Wkly Rep 2015;64:1078–82. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources