

Evaluation of a Bayesian penalized likelihood reconstruction algorithm for low-count clinical 18F-FDG PET/CT
- PMID: 31889228
- PMCID: PMC6937357
- DOI: 10.1186/s40658-019-0262-y
Evaluation of a Bayesian penalized likelihood reconstruction algorithm for low-count clinical 18F-FDG PET/CT
Abstract
Background: Recently, a Bayesian penalized likelihood (BPL) reconstruction algorithm was introduced for a commercial PET/CT with the potential to improve image quality. We compared the performance of this BPL algorithm with conventional reconstruction algorithms under realistic clinical conditions such as daily practiced at many European sites, i.e. low 18F-FDG dose and short acquisition times.
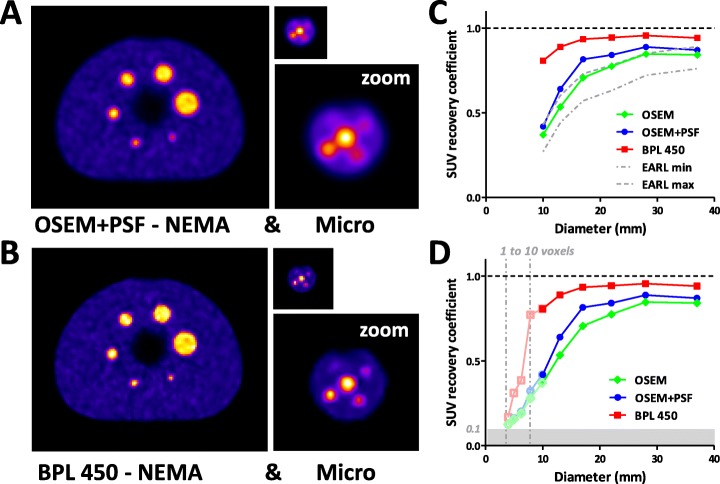
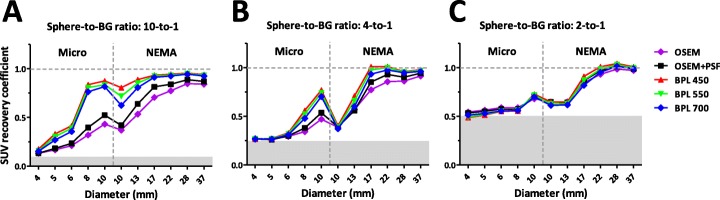
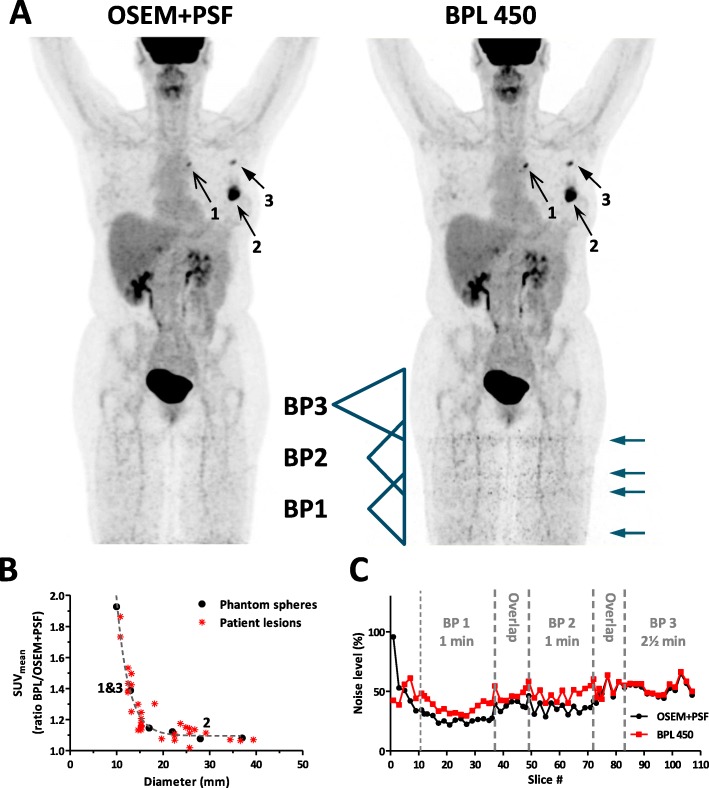
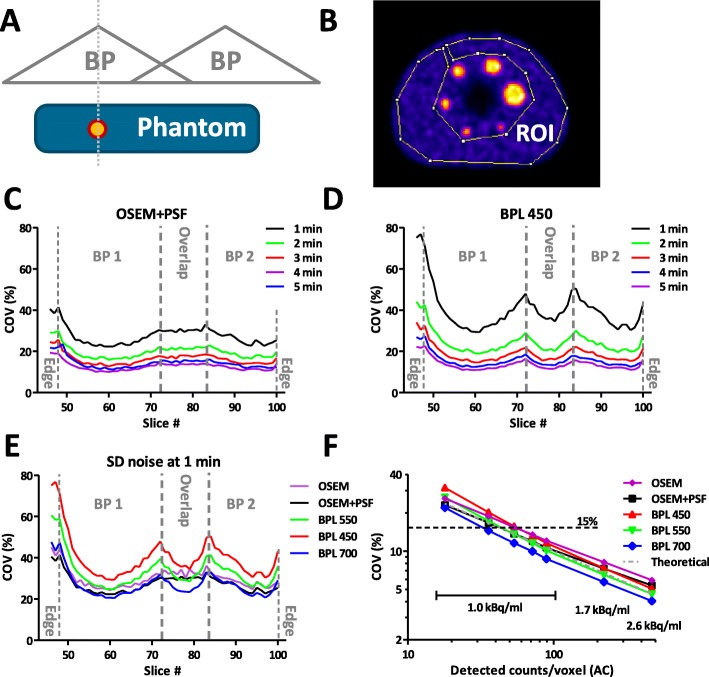
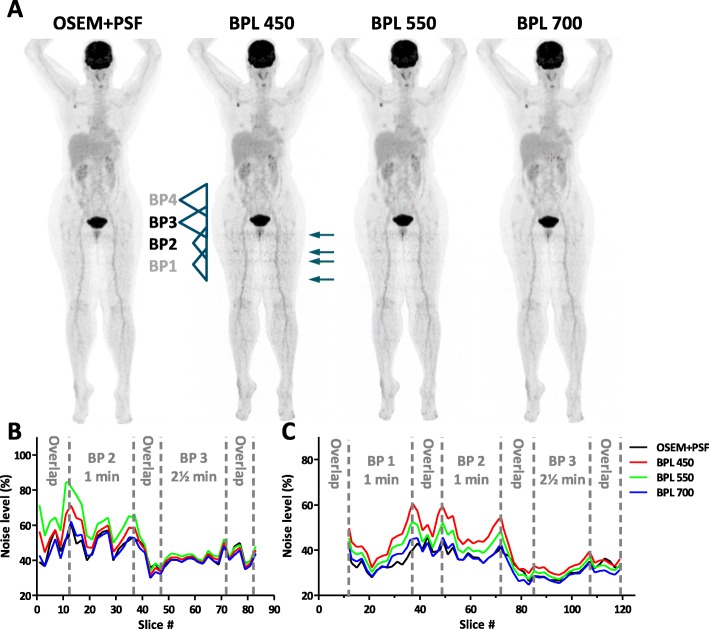
Results: To study the performance of the BPL algorithm, regular clinical 18F-FDG whole body PET scans were made. In addition, two types of phantoms were scanned with 4-37 mm sized spheres filled with 18F-FDG at sphere-to-background ratios of 10-to-1, 4-to-1, and 2-to-1. Images were reconstructed using standard ordered-subset expectation maximization (OSEM), OSEM with point spread function (PSF), and the BPL algorithm using β-values of 450, 550 and 700. To quantify the image quality, the lesion detectability, activity recovery, and the coefficient of variation (COV) within a single bed position (BP) were determined. We found that when applying the BPL algorithm both smaller lesions in clinical studies as well as spheres in phantom studies can be detected more easily due to a higher SUV recovery, especially for higher contrast ratios. Under standard clinical scanning conditions, i.e. low number of counts, the COV is higher for the BPL (β=450) than the OSEM+PSF algorithm. Increase of the β-value to 550 or 700 results in a COV comparable to OSEM+PSF, however, at the cost of contrast, though still better than OSEM+PSF. At the edges of the axial field of view (FOV) where BPs overlap, COV can increase to levels at which bands become visible in clinical images, related to the lower local axial sensitivity of the PET/CT, which is due to the limited bed overlap of 23% such as advised by the manufacturer.
Conclusions: The BPL algorithm performs better than the standard OSEM+PSF algorithm on small lesion detectability, SUV recovery, and noise suppression. Increase of the percentage of bed overlap, time per BP, administered activity, or the β-value, all have a direct positive impact on image quality, though the latter with some loss of small lesion detectability. Thus, BPL algorithms are very interesting for improving image quality, especially in small lesion detectability.
Keywords: Bayesian penalized likelihood; Micro Hollow Sphere phantom; NEMA image quality phantom; Q.Clear; image quality; image reconstruction; optimization; positron emission tomography.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
