

Use of air stacking to improve pulmonary function in Indonesian Duchenne muscular dystrophy patients: bridging the standard of care gap in low middle income country setting
- PMID: 31890014
- PMCID: PMC6912939
- DOI: 10.1186/s12919-019-0179-4
Use of air stacking to improve pulmonary function in Indonesian Duchenne muscular dystrophy patients: bridging the standard of care gap in low middle income country setting
Abstract
Background: Duchenne Muscular Dystrophy (DMD) is a fatal X-linked recessive neuromuscular disease, characterized by progressive loss of muscle strength. Respiratory failure is the main cause of morbidity and mortality in DMD patients. Respiratory devices have been reported to increase the effectiveness of cough and pulmonary function, thus prolong the survival rate. However, there is scarcity of studies about DMD patients' respiratory profiles and usage of respiratory devices in Indonesia.
Methods: We recruited 8 Indonesian DMD patients in Dr. Sardjito Hospital and UGM Academic Hospital, Yogyakarta. Baseline pulmonary function was measured using spirometry. Peak Cough Flow was measured at baseline, with chest compression, after air stacking with manual ventilation bag, and with the combined techniques. Data recorded was presented as mean ± SD and analysed using ANOVA.
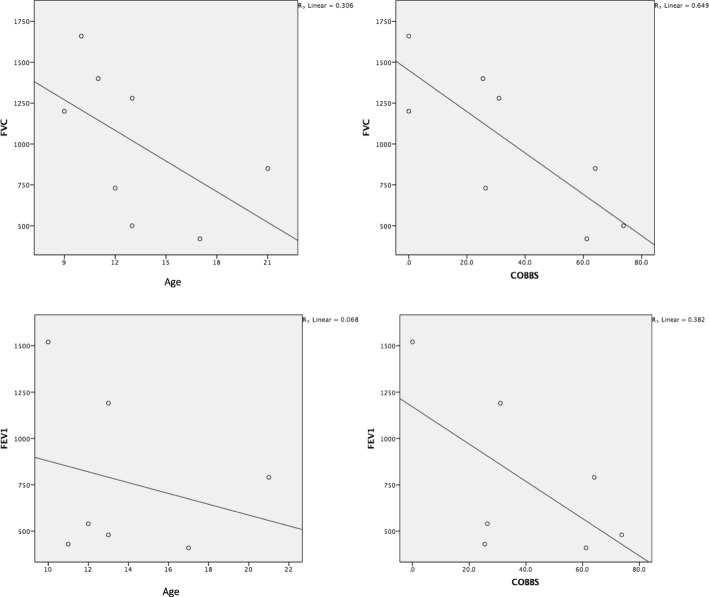
Results: Here we show the respiratory profiles from 8 non-ambulatory DMD patients (mean age: 13.25 ± 3.96 years old) confirmed by genetic testing. None of them had access to respiratory devices. Spirometry measurements showed 7 of 8 patients had severe restrictive pulmonary function with mean FEV1/FVC 22.40 ± 10.30% of predictive values (normal ratio > 70%). In addition, all patients showed poor cough performances measured by peak cough flowmeter (160 ± 44.58 L/min (normal value > 270 L/min)) that were improved by air stacking using a manual ventilation bag (167.4 ± 46.72 L/min). Three patients who had nocturnal hypoventilation did not have daytime hypercapnia. Manual ventilation bag or mechanical in-/ex-sufflation was indicated in 75% of patients while nocturnal assisted ventilation was indicated in 50% of patients. Neither daytime assisted ventilation nor tracheostomy was indicated in these patients.
Conclusion: Use of manual exsufflation in combination with the manual ventilation bag for air stacking to improve cough performance is recommended as the first step of respiratory management in DMD patients. Provision of manual ventilation bag serve as an affordable and effective device for respiratory support in the early stage of respiratory involvement in those non-ambulatory patients with DMD.
Keywords: Duchenne muscular dystrophy; Respiratory devices; Respiratory function.
© The Author(s). 2019.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures

References
-
- Sheehan Daniel W., Birnkrant David J., Benditt Joshua O., Eagle Michelle, Finder Jonathan D., Kissel John, Kravitz Richard M., Sawnani Hemant, Shell Richard, Sussman Michael D., Wolfe Lisa F. Respiratory Management of the Patient With Duchenne Muscular Dystrophy. Pediatrics. 2018;142(Supplement 2):S62–S71. doi: 10.1542/peds.2018-0333H. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
