

doi: 10.1016/j.eats.2019.06.020.
eCollection 2019 Nov.
Arthroscopic Posterior Glenohumeral Capsular Augmentation With Gracilis Tendon Allograft
Affiliations
- PMID: 31890495
- PMCID: PMC6926306
- DOI: 10.1016/j.eats.2019.06.020
Item in Clipboard
Arthroscopic Posterior Glenohumeral Capsular Augmentation With Gracilis Tendon Allograft
Arthrosc Tech.
.
Abstract
Recurrent shoulder instability complicated by capsular insufficiency due to underlying soft-tissue disorders or multiple prior failed surgical procedures poses a challenging surgical problem. Traditional capsulolabral soft-tissue reconstruction techniques are less effective in this setting, and bony procedures sacrifice normal anatomic relations. The described arthroscopic technique aims to prevent instability while maintaining range of motion through creation of a soft-tissue allograft "sling" augmenting the posterior glenohumeral capsule.
© 2019 by the Arthroscopy Association of North America. Published by Elsevier.
Figures

The gracilis tendon allograft, no greater than 5 mm in diameter, is trimmed to 65 mm in total length with whipstitches (FiberLoop) on both ends and a single suture in a luggage-tag configuration (FiberLink) at the midpoint to form the apex. The end FiberLoops are anchored to the glenoid, and the apex FiberLink is anchored to the humeral head. Different suture coloration schemes should be selected for each suture to aid in identification during the procedure.

Right shoulder with patient in lateral decubitus position and an anterior viewing portal. A 2.9-mm PushLock suture anchor is placed into the joint through a percutaneous cannula using an accessory posterolateral portal (i.e. portal of Wilmington). A left curved SutureLasso is brought into the joint through the Gemini cannula in the posterior portal and used to pass a nitinol wire loop through the PushLock eyelet. The nitinol wire is then retrieved through the posterior portal and used to shuttle the graft FiberLoop suture through the eyelet in preparation for anchoring at the glenoid.

Right shoulder with patient in lateral decubitus position. The graft is shuttled into the joint through the Gemini cannula in the posterior portal. The camera is in the anterior portal, and a 2.9-mm PushLock suture anchor is held in the joint space through a posterolateral accessory portal with a percutaneous cannula.

Right shoulder with patient in lateral decubitus position and anterior viewing portal. With the graft shuttled into the joint using suture through the eyelet of the 2.9-mm PushLock suture anchor, the graft is anchored into the pilot hole created at the posterior-inferior glenoid.

Right shoulder with patient in lateral decubitus position and anterior viewing portal. The second end of the graft is anchored into the mid-posterior glenoid using a second 2.9-mm PushLock suture anchor.
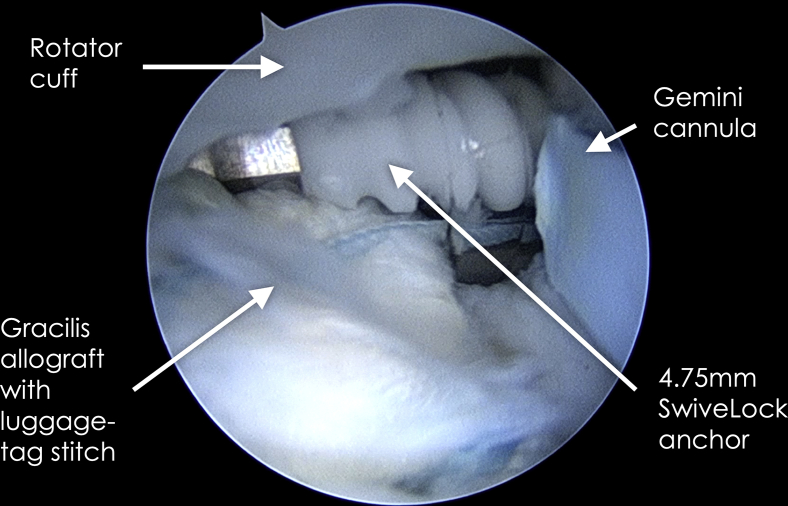
Right shoulder with patient in lateral decubitus position and anterior viewing portal. The apex of the graft is anchored to the posterior humeral head at the articular margin using a 4.75-mm SwiveLock anchor and the FiberLink suture previously placed at the graft's apex.

Right shoulder with patient in lateral decubitus position and anterior viewing portal. The final graft configuration is an inverse V, with either end anchored to the glenoid and the apex anchored to the humeral head. Anchor points are labeled with yellow text and arrows.
References
-
- Vavken P., Tepolt F.A., Kocher M.S. Open inferior capsular shift for multidirectional shoulder instability in adolescents with generalized ligamentous hyperlaxity or Ehlers-Danlos syndrome. J Shoulder Elbow Surg. 2016;25:907–912. - PubMed
-
- Latarjet M. [Treatment of recurrent dislocation of the shoulder] Lyon Chir. 1954;49:994–997. [in French] - PubMed
-
- Joshi M.A., Young A.A., Balestro J.C., Walch G. The Latarjet-Patte procedure for recurrent anterior shoulder instability in contact athletes. Orthop Clin North Am. 2015;46:105–111. - PubMed
-
- Marion B., Klouche S., Deranlot J., Bauer T., Nourissat G., Hardy P. A prospective comparative study of arthroscopic versus mini-open Latarjet procedure with a minimum 2-year follow-up. Arthroscopy. 2017;33:269–277. - PubMed
LinkOut - more resources
Full Text Sources
