

Bipolar Fresh Osteochondral Allograft Transplantation and Joint Reconstruction for Patellar and Trochlear Cartilage Defects
- PMID: 31890534
- PMCID: PMC6928370
- DOI: 10.1016/j.eats.2019.08.003
Bipolar Fresh Osteochondral Allograft Transplantation and Joint Reconstruction for Patellar and Trochlear Cartilage Defects
Abstract
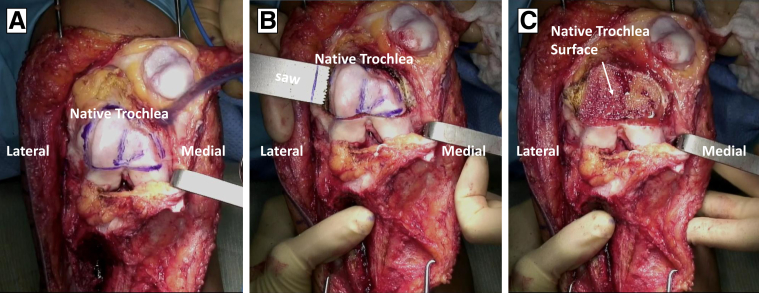
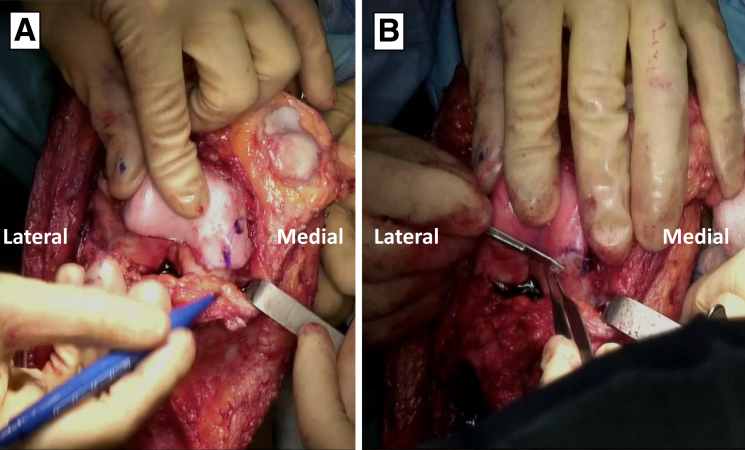
Patellar instability is a debilitating condition, and trauma due to the dislocations may severely damage the articular cartilage of the patellofemoral joint. The lack of healing capacity of cartilage makes treatment of such lesions challenging. In young patients, preservation of native bone and cartilage is a priority, and therefore arthroplasty procedures should be avoided even in relatively larger lesions. Fresh osteochondral allografting has been described for these difficult and complex cases, with recent studies showing promising results. In this surgical technique, we describe the use of bipolar osteochondral allografts of the patella and trochlea and patellofemoral joint reconstruction for large bipolar full-thickness cartilage defects due to recurrent dislocation events.
© 2019 Published by Elsevier on behalf of the Arthroscopy Association of North America.
Figures













Similar articles
-
Bipolar Osteochondral Allograft Transplantation of the Patella and Trochlea.Cartilage. 2020 Oct;11(4):431-440. doi: 10.1177/1947603518796124. Epub 2018 Sep 3. Cartilage. 2020. PMID: 30173540 Free PMC article.
-
Treatment of "patellofemoral" cartilage lesions with matrix-assisted autologous chondrocyte transplantation: a comparison of patellar and trochlear lesions.Am J Sports Med. 2014 Mar;42(3):626-34. doi: 10.1177/0363546513510884. Epub 2013 Dec 3. Am J Sports Med. 2014. PMID: 24302700
-
The Effect of Patellar Surface Morphology on Subchondral Bone Alignment When Matching Patellar Osteochondral Allografts to the Central Ridge of the Patella.Am J Sports Med. 2022 May;50(6):1635-1643. doi: 10.1177/03635465221087391. Epub 2022 Apr 19. Am J Sports Med. 2022. PMID: 35438027
-
Use of Fresh Osteochondral Allografts in the Patellofemoral Joint.J Knee Surg. 2018 Mar;31(3):227-230. doi: 10.1055/s-0037-1607324. Epub 2017 Oct 16. J Knee Surg. 2018. PMID: 29036755 Review.
-
Clinical Outcomes and Failure Rates of Osteochondral Allograft Transplantation in the Knee: A Systematic Review.Am J Sports Med. 2018 Dec;46(14):3541-3549. doi: 10.1177/0363546517732531. Epub 2017 Oct 17. Am J Sports Med. 2018. PMID: 29039969
Cited by
-
Osteochondral Allograft Transplant for Combined Medial and Lateral Patellar Cartilage Lesions: The Osteochondral Wide Lesion (OWL) Technique.Arthrosc Tech. 2022 Oct 20;11(11):e1963-e1972. doi: 10.1016/j.eats.2022.07.012. eCollection 2022 Nov. Arthrosc Tech. 2022. PMID: 36457384 Free PMC article.
References
-
- Christensen T.C., Sanders T.L., Pareek A., Mohan R., Dahm D.L., Krych A.J. Risk factors and time to recurrent ipsilateral and contralateral patellar dislocations. Am J Sports Med. 2017;45:2105–2110. - PubMed
-
- Sanders T.L., Pareek A., Hewett T.E., Stuart M.J., Dahm D.L., Krych A.J. High rate of recurrent patellar dislocation in skeletally immature patients: A long-term population-based study. Knee Surg Sports Traumatol Arthrosc. 2018;26:1037–1043. - PubMed
-
- Weber A.E., Nathani A., Dines J.S. An algorithmic approach to the management of recurrent lateral patellar dislocation. J Bone Joint Surg Am. 2016;98:417–427. - PubMed
-
- Mankin H.J. The response of articular cartilage to mechanical injury. J Bone Joint Surg Am. 1982;64:460–466. - PubMed
-
- Meric G., Gracitelli G.C., Görtz S., De Young A.J., Bugbee W.D. Fresh osteochondral allograft transplantation for bipolar reciprocal osteochondral lesions of the knee. Am J Sports Med. 2015;43:709–714. - PubMed
LinkOut - more resources
Full Text Sources
