

Diagnosis and Treatment of Keloids and Hypertrophic Scars-Japan Scar Workshop Consensus Document 2018
- PMID: 31890718
- PMCID: PMC6933735
- DOI: 10.1186/s41038-019-0175-y
Diagnosis and Treatment of Keloids and Hypertrophic Scars-Japan Scar Workshop Consensus Document 2018
Abstract
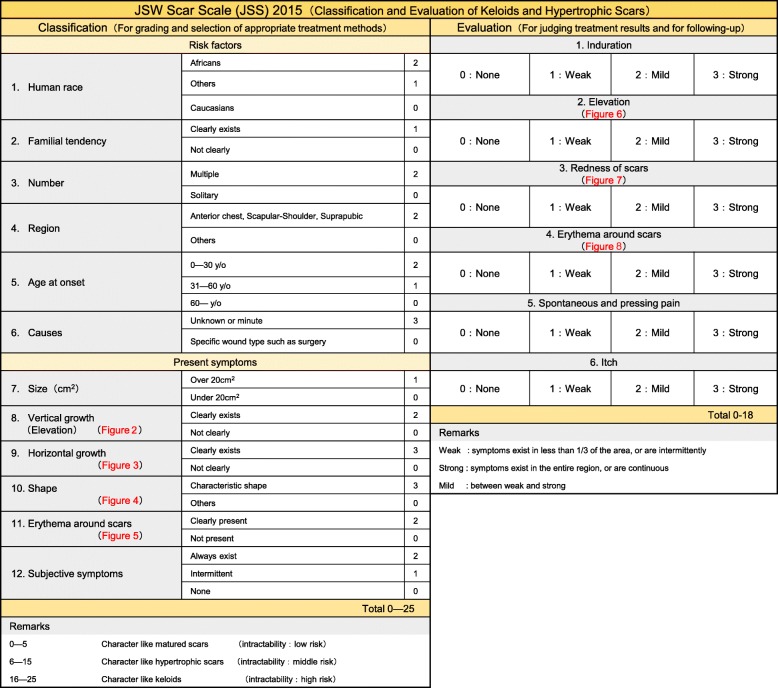
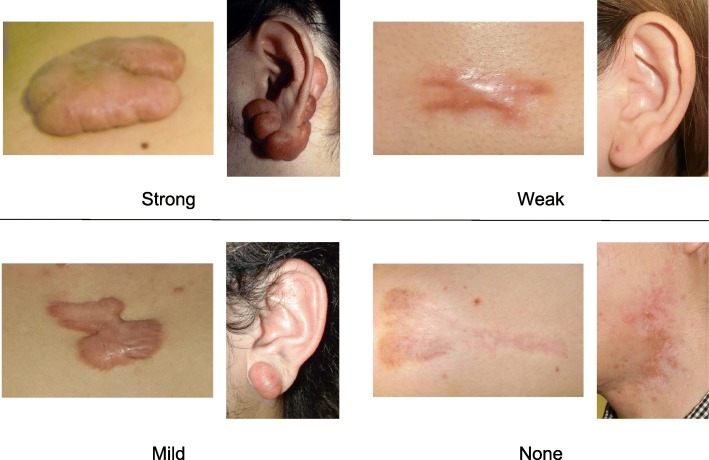
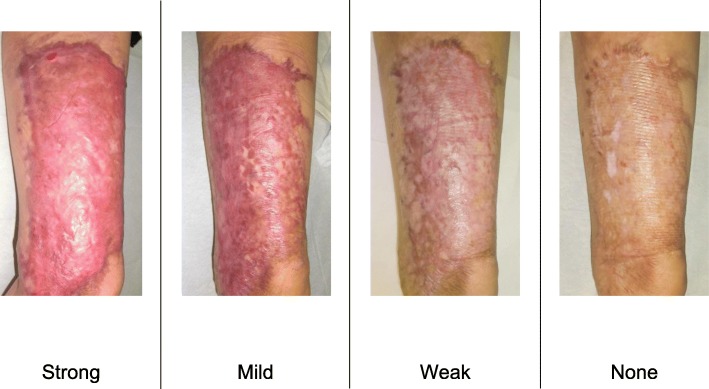
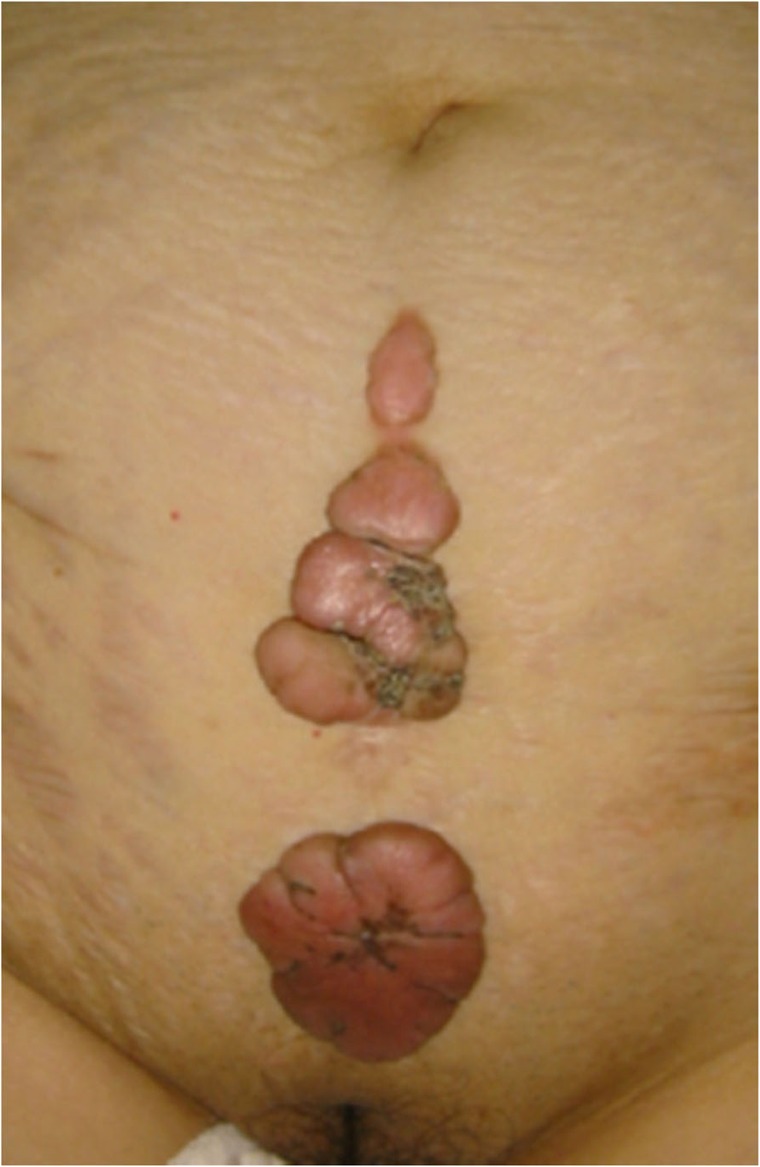
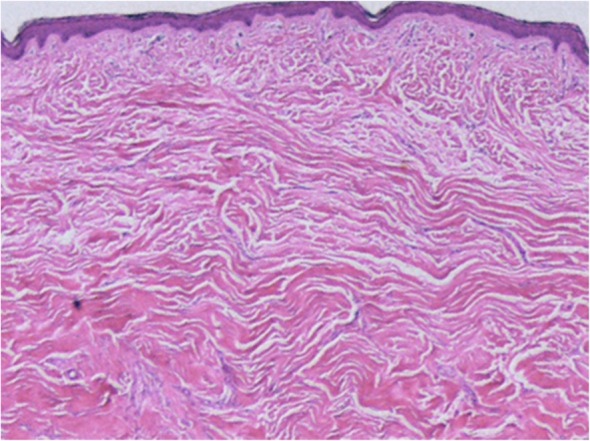
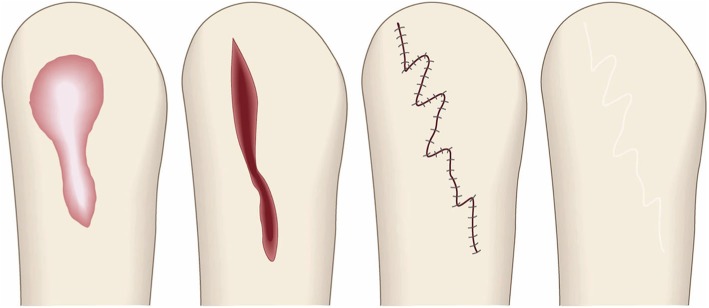
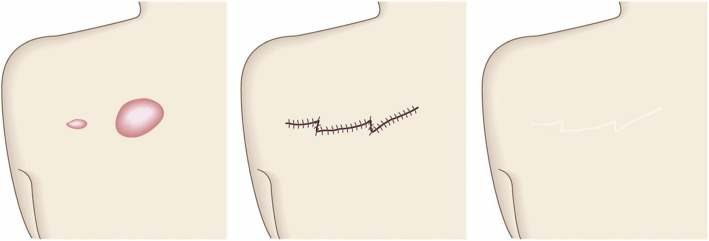
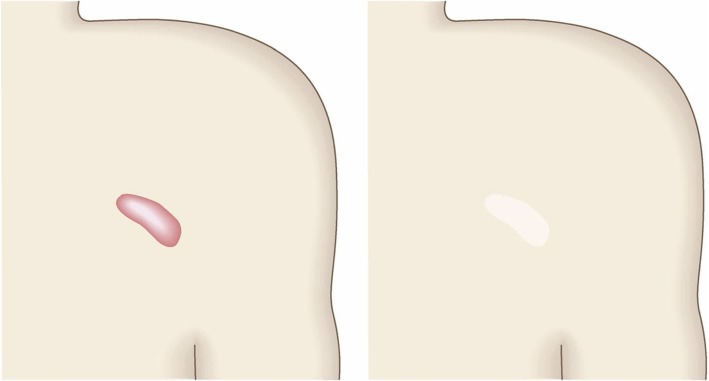
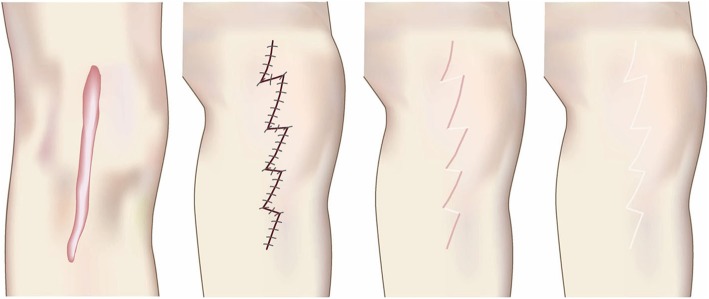
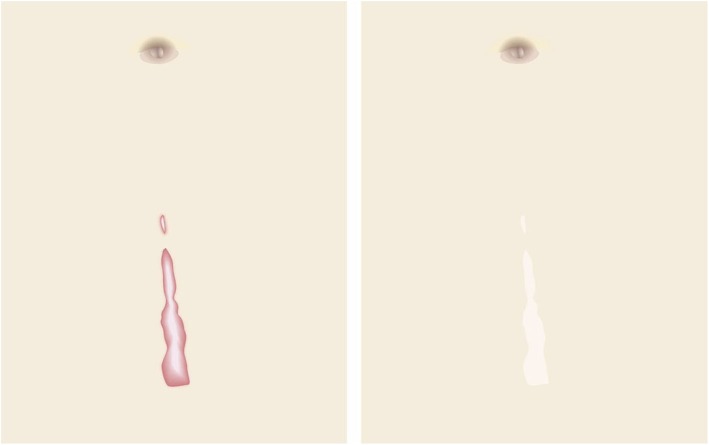
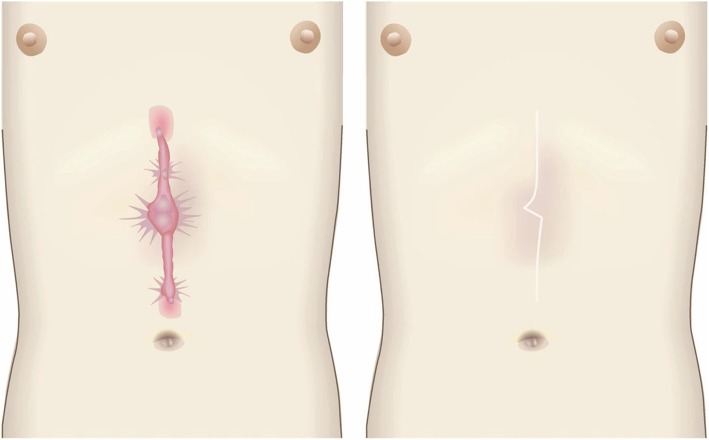
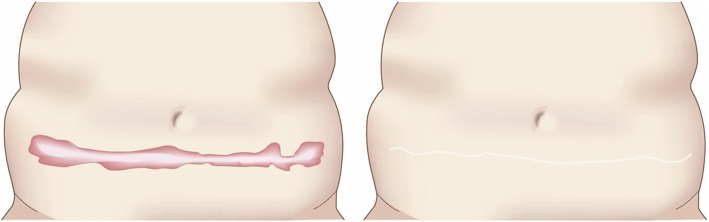
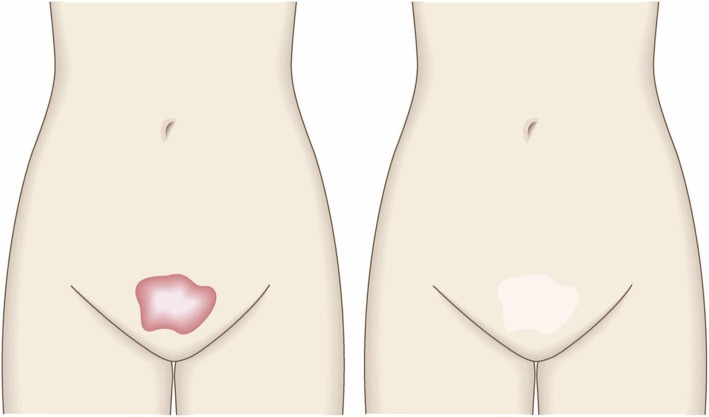
There has been a long-standing need for guidelines on the diagnosis and treatment of keloids and hypertrophic scars that are based on an understanding of the pathomechanisms that underlie these skin fibrotic diseases. This is particularly true for clinicians who deal with Asian and African patients because these ethnicities are highly prone to these diseases. By contrast, Caucasians are less likely to develop keloids and hypertrophic scars, and if they do, the scars tend not to be severe. This ethnic disparity also means that countries vary in terms of their differential diagnostic algorithms. The lack of clear treatment guidelines also means that primary care physicians are currently applying a hotchpotch of treatments, with uneven outcomes. To overcome these issues, the Japan Scar Workshop (JSW) has created a tool that allows clinicians to objectively diagnose and distinguish between keloids, hypertrophic scars, and mature scars. This tool is called the JSW Scar Scale (JSS) and it involves scoring the risk factors of the individual patients and the affected areas. The tool is simple and easy to use. As a result, even physicians who are not accustomed to keloids and hypertrophic scars can easily diagnose them and judge their severity. The JSW has also established a committee that, in cooperation with outside experts in various fields, has prepared a Consensus Document on keloid and hypertrophic scar treatment guidelines. These guidelines are simple and will allow even inexperienced clinicians to choose the most appropriate treatment strategy. The Consensus Document is provided in this article. It describes (1) the diagnostic algorithm for pathological scars and how to differentiate them from clinically similar benign and malignant tumors, (2) the general treatment algorithms for keloids and hypertrophic scars at different medical facilities, (3) the rationale behind each treatment for keloids and hypertrophic scars, and (4) the body site-specific treatment protocols for these scars. We believe that this Consensus Document will be helpful for physicians from all over the world who treat keloids and hypertrophic scars.
Keywords: Guideline; Hypertrophic scars; Keloid; Laser; Pathological scars; Pathology; Radiotherapy; Steroid; Surgery.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures














References
-
- Ogawa R, Akaishi S, Akita S, Okabe K, Shimizu T, Sunaga A, et al. Japan Scar Workshop (JSW) Scar Scale 2015. Available online at; http://www.scar-keloid.com/pdf/JSW_scar_scale_2015_EN.pdf. Accessed 1 Oct 2019.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
