

Global variation in anastomosis and end colostomy formation following left-sided colorectal resection
- PMID: 31891112
- PMCID: PMC6921967
- DOI: 10.1002/bjs5.50138
Global variation in anastomosis and end colostomy formation following left-sided colorectal resection
Abstract
Background: End colostomy rates following colorectal resection vary across institutions in high-income settings, being influenced by patient, disease, surgeon and system factors. This study aimed to assess global variation in end colostomy rates after left-sided colorectal resection.
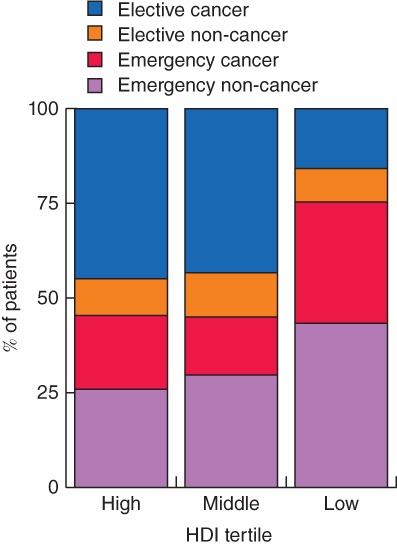
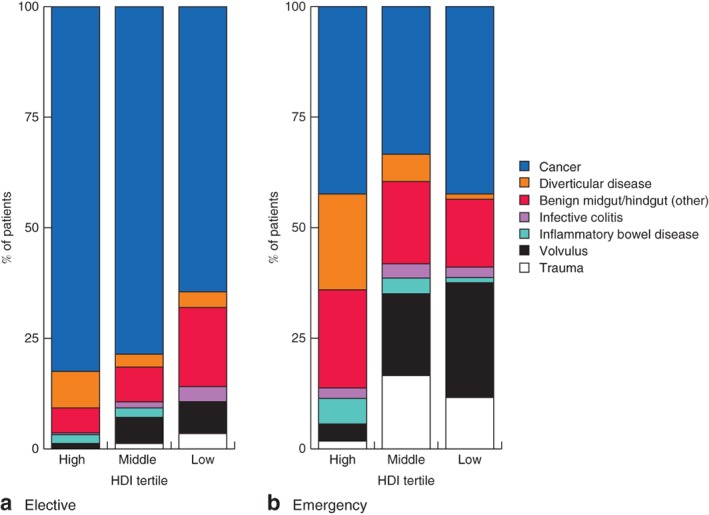
Methods: This study comprised an analysis of GlobalSurg-1 and -2 international, prospective, observational cohort studies (2014, 2016), including consecutive adult patients undergoing elective or emergency left-sided colorectal resection within discrete 2-week windows. Countries were grouped into high-, middle- and low-income tertiles according to the United Nations Human Development Index (HDI). Factors associated with colostomy formation versus primary anastomosis were explored using a multilevel, multivariable logistic regression model.
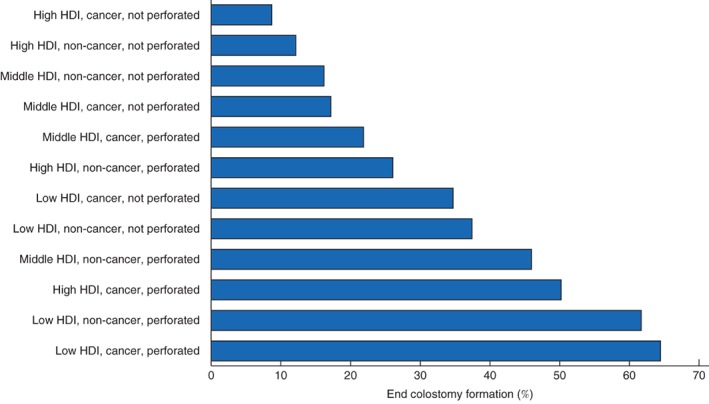
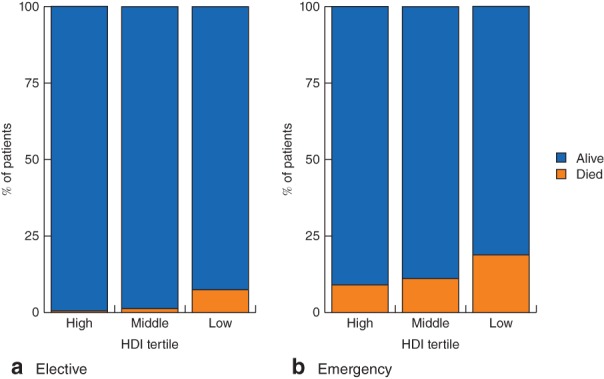
Results: In total, 1635 patients from 242 hospitals in 57 countries undergoing left-sided colorectal resection were included: 113 (6·9 per cent) from low-HDI, 254 (15·5 per cent) from middle-HDI and 1268 (77·6 per cent) from high-HDI countries. There was a higher proportion of patients with perforated disease (57·5, 40·9 and 35·4 per cent; P < 0·001) and subsequent use of end colostomy (52·2, 24·8 and 18·9 per cent; P < 0·001) in low- compared with middle- and high-HDI settings. The association with colostomy use in low-HDI settings persisted (odds ratio (OR) 3·20, 95 per cent c.i. 1·35 to 7·57; P = 0·008) after risk adjustment for malignant disease (OR 2·34, 1·65 to 3·32; P < 0·001), emergency surgery (OR 4·08, 2·73 to 6·10; P < 0·001), time to operation at least 48 h (OR 1·99, 1·28 to 3·09; P = 0·002) and disease perforation (OR 4·00, 2·81 to 5·69; P < 0·001).
Conclusion: Global differences existed in the proportion of patients receiving end stomas after left-sided colorectal resection based on income, which went beyond case mix alone.
© 2019 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Comment in
-
Comment on: Global variation in anastomosis and end colostomy formation following left-sided colorectal resection.BJS Open. 2021 May 7;5(3):zrab045. doi: 10.1093/bjsopen/zrab045. BJS Open. 2021. PMID: 34021329 Free PMC article.
-
Stoma care research in low- and middle-income countries: update from the NIHR global health research unit on global surgery.BJS Open. 2021 May 7;5(3):zrab046. doi: 10.1093/bjsopen/zrab046. BJS Open. 2021. PMID: 34037697 Free PMC article. No abstract available.
References
-
- Sullivan R, Alatise OI, Anderson BO, Audisio R, Autier P, Aggarwal A et al. Global cancer surgery: delivering safe, affordable, and timely cancer surgery. Lancet Oncol 2015; 16: 1193–1224. - PubMed
-
- GlobalSurg Collaborative . Mortality of emergency abdominal surgery in high‐, middle‐ and low‐income countries. Br J Surg 2016; 103: 971–988. - PubMed
-
- Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017; 66: 683–691. - PubMed
-
- Morris E, Quirke P, Thomas JD, Fairley L, Cottier B, Forman D. Unacceptable variation in abdominoperineal excision rates for rectal cancer: time to intervene? Gut 2008; 57: 1690–1697. - PubMed
-
- Thyø A, Emmertsen KJ, Pinkney TD, Christensen P, Laurberg S. The colostomy impact score: development and validation of a patient reported outcome measure for rectal cancer patients with a permanent colostomy. A population‐based study. Colorectal Dis 2017; 19: O25–O33. - PubMed
