

Impact of aromatase inhibitor treatment on global gene expression and its association with antiproliferative response in ER+ breast cancer in postmenopausal patients
- PMID: 31892336
- PMCID: PMC6938628
- DOI: 10.1186/s13058-019-1223-z
Impact of aromatase inhibitor treatment on global gene expression and its association with antiproliferative response in ER+ breast cancer in postmenopausal patients
Abstract
Background: Endocrine therapy reduces breast cancer mortality by 40%, but resistance remains a major clinical problem. In this study, we sought to investigate the impact of aromatase inhibitor (AI) therapy on gene expression and identify gene modules representing key biological pathways that relate to early AI therapy resistance.
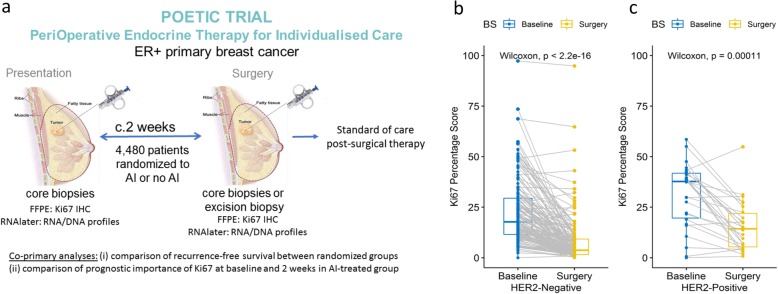
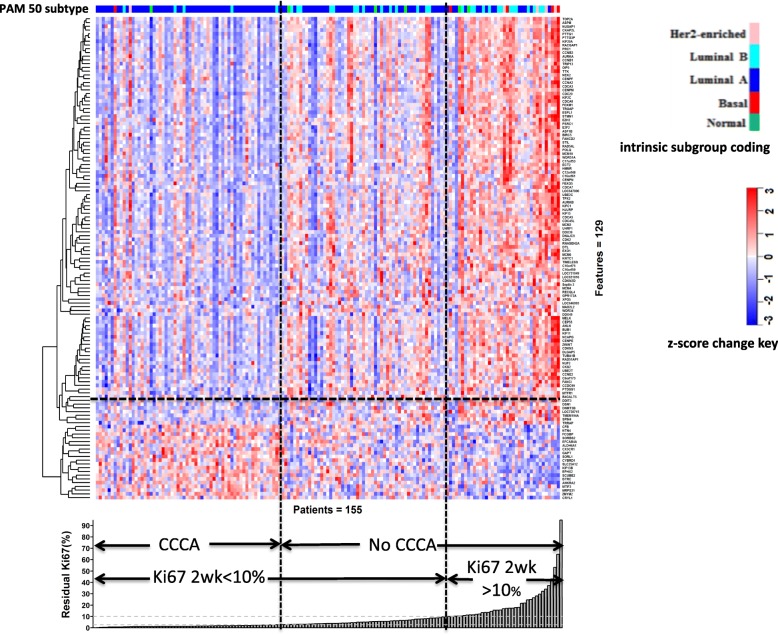
Methods: Global gene expression was measured on pairs of core-cut biopsies taken at baseline and at surgery from 254 patients with ER-positive primary breast cancer randomised to receive 2-week presurgical AI (n = 198) or no presurgical treatment (control n = 56) from the POETIC trial. Data from the AI group was adjusted to eliminate artefactual process-related changes identified in the control group. The response was assessed by changes in the proliferation marker, Ki67.
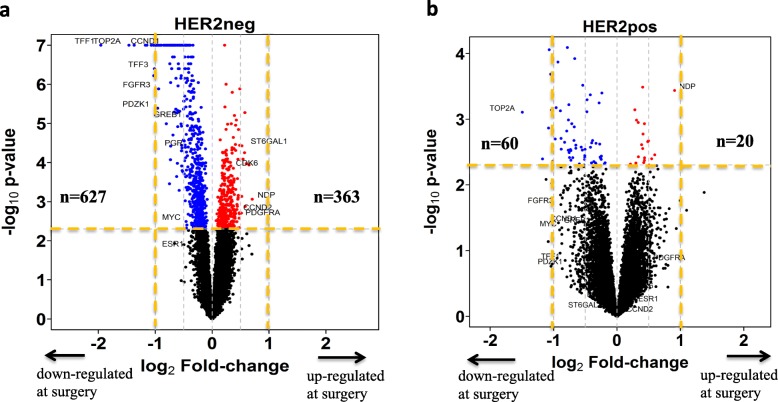
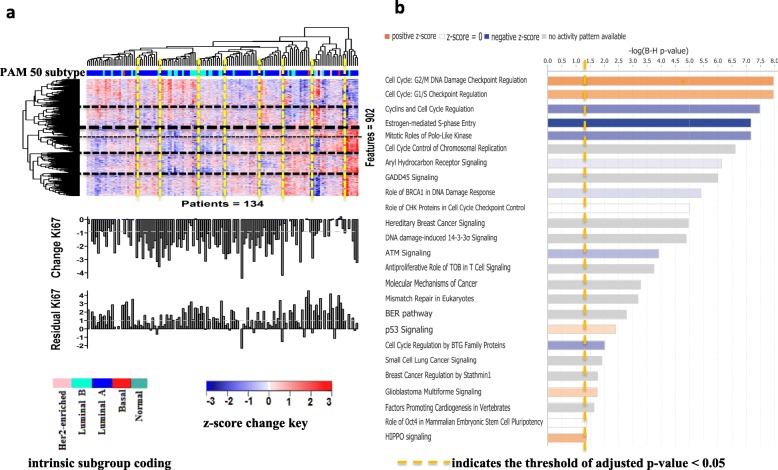
Results: High baseline ESR1 expression associated with better AI response in HER2+ tumours but not HER2- tumours. In HER2- tumours, baseline expression of 48 genes associated with poor antiproliferative response (p < 0.005) including PERP and YWHAQ, the two most significant, and the transcription co-regulators (SAP130, HDAC4, and NCOA7) which were among the top 16 most significant. Baseline gene signature scores measuring cell proliferation, growth factor signalling (ERBB2-GS, RET/GDNF-GS, and IGF-1-GS), and immune activity (STAT1-GS) were significantly higher in poor AI responders. Two weeks of AI caused downregulation of genes involved in cell proliferation and ER signalling, as expected. Signature scores of E2F activation and TP53 dysfunction after 2-week AI were associated with poor AI response in both HER2- and HER2+ patients.
Conclusions: There is a high degree of heterogeneity in adaptive mechanisms after as little as 2-week AI therapy; however, all appear to converge on cell cycle regulation. Our data support the evaluation of whether an E2F signatures after short-term exposure to AI may identify those patients most likely to benefit from the early addition of CDK4/6 inhibitors.
Trial registration: ISRCTN, ISRCTN63882543, registered on 18 December 2007.
Keywords: Aromatase inhibition; Breast cancer; Oestrogen receptor; Residual proliferation; Resistance; Signatures.
Conflict of interest statement
MD and LAM receive academic funding from Pfizer, Puma Biotechnology Inc., and AstraZeneca. MD receives honoraria from Myriad Genetics and speaker’s bureau of Roche; is a consultant and advisory board member of Radius, GTx, and Orion Pharma; and has received remuneration from the ICR rewards to Inventors Schemes. MCUC has a patent: US Patent No. 9,631,239 with royalties paid. All other authors declare that they have no competing interests.
Figures
References
-
- Dodson A, Parry S, Ibrahim M, Bartlett JM, Pinder S, Dowsett M, et al. Breast cancer biomarkers in clinical testing: analysis of a UK national external quality assessment scheme for immunocytochemistry and in situ hybridisation database containing results from 199 300 patients. J Pathol Clin Res. 2018;4(4):262–273. doi: 10.1002/cjp2.112. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
