

CSF biomarkers of neuroinflammation in distinct forms and subtypes of neurodegenerative dementia
- PMID: 31892365
- PMCID: PMC6937795
- DOI: 10.1186/s13195-019-0562-4
CSF biomarkers of neuroinflammation in distinct forms and subtypes of neurodegenerative dementia
Abstract
Background: In neurodegenerative dementias (NDs) such as prion disease, Alzheimer's disease (AD), and frontotemporal lobar degeneration (FTLD), protein misfolding leads to the tissue deposition of protein aggregates which, in turn, trigger neuroinflammation and neurodegeneration. Cerebrospinal fluid (CSF) biomarkers have the potential to reflect different aspects of these phenomena across distinct clinicopathological subtypes and disease stages.
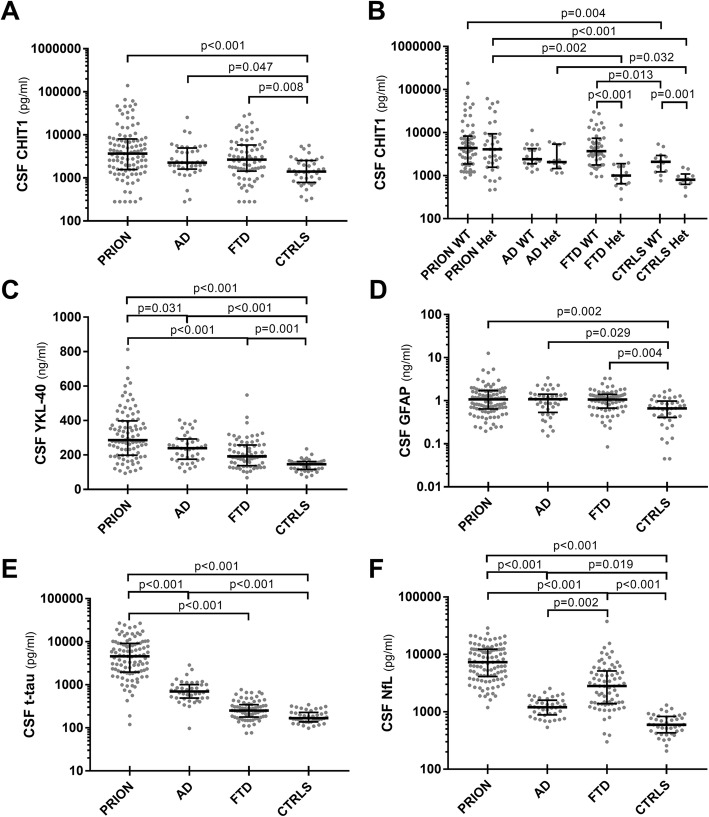
Methods: We investigated CSF glial markers, namely chitotriosidase 1 (CHIT1), chitinase-3-like protein 1 (YKL-40) and glial fibrillary acidic protein (GFAP) in prion disease subtypes (n = 101), AD (n = 40), clinicopathological subgroups of FTLD (n = 72), and controls (n = 40) using validated, commercially available ELISA assays. We explored glial biomarker levels' associations with disease variables and neurodegenerative CSF biomarkers and evaluated their diagnostic accuracy. The genotype of the CHIT1 rs3831317 polymorphic site was also analyzed.
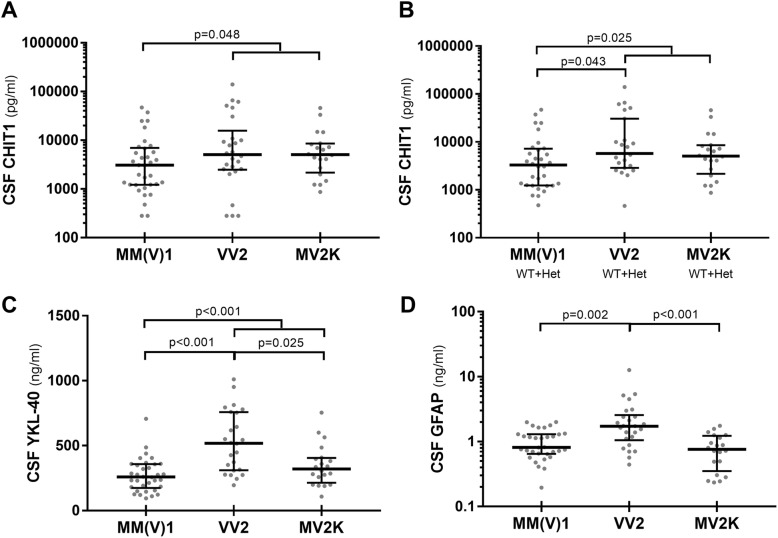
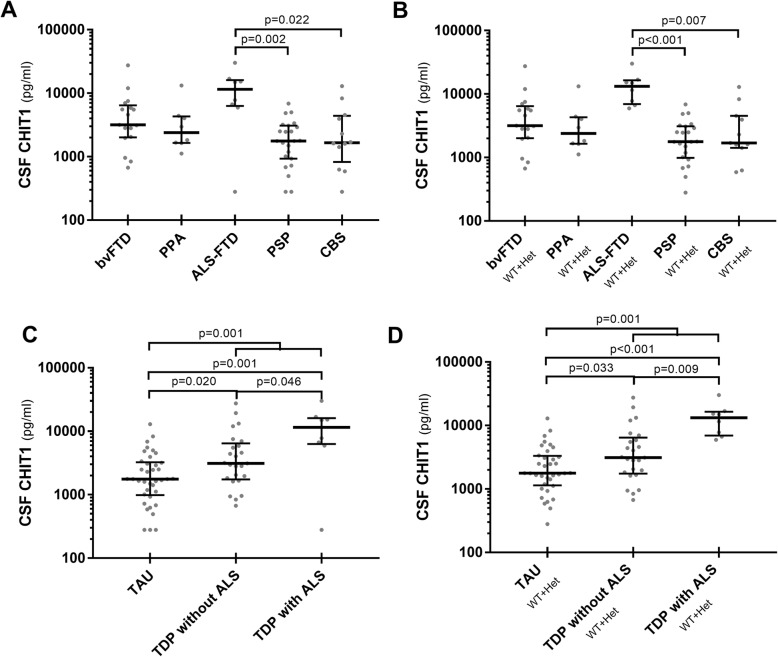
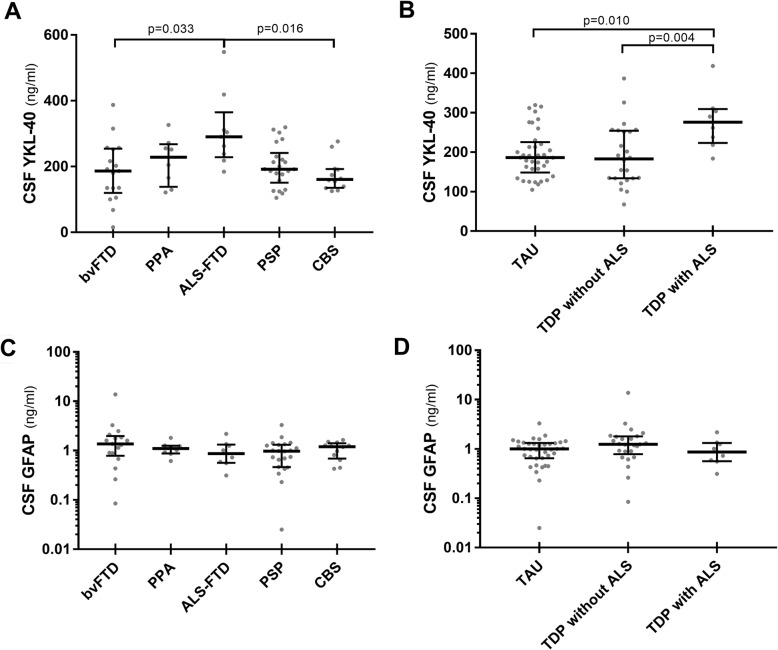
Results: Each ND group showed increased levels of CHIT1, YKL-40, and GFAP compared to controls with a difference between prion disease and AD or FTLD limited to YKL-40, which showed higher values in the former group. CHIT1 levels were reduced in both heterozygotes and homozygotes for the CHIT1 24-bp duplication (rs3831317) in FTLD and controls, but this effect was less significant in AD and prion disease. After stratification according to molecular subgroups, we demonstrated (i) an upregulation of all glial markers in Creutzfeldt-Jakob disease VV2 compared to other disease subtypes, (ii) a difference in CHIT1 levels between FTLD with TAU and TDP43 pathology, and (iii) a marked increase of YKL-40 in FTLD with amyotrophic lateral sclerosis (ALS) in comparison with FTLD without ALS. In prion disease, glial markers correlated with disease stage and were already elevated in one pre-symptomatic case of Gerstmann-Sträussler-Scheinker disease. Regarding the diagnostic value, YKL-40 was the only glial marker that showed a moderate accuracy in the distinction between controls and NDs.
Conclusions: NDs share a CSF profile characterized by increased levels of CSF CHIT1, YKL-40, and GFAP, which likely reflects a common neuroinflammatory response to protein misfolding and aggregation. CSF glial markers of neuroinflammation demonstrate limited diagnostic value but have some potential for monitoring the clinical and, possibly, preclinical phases of NDs.
Keywords: Alzheimer’s disease; Amyloid-beta; Amyotrophic lateral sclerosis; Corticobasal syndrome; Creutzfeldt-Jakob disease; Frontotemporal dementia; Human prion disease; Neurofilament light; Progressive supranuclear palsy; Tau protein.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- "Ricerca Corrente"/Ministero della Salute/International
- FTLDc O1GI1007A/Bundesministerium für Bildung und Forschung/International
- MR/J016071/1/MRC_/Medical Research Council/United Kingdom
- SOPHIA (01ED1202A), BiomarkAPD (01ED1203F) and Prefrontals (01ED1512)/EU Joint Programme - Neurodegenerative Disease Research/International
- ETM/58/CSO_/Chief Scientist Office/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
