

Life Expectancy of Adult Survivors of Childhood Cancer Over 3 Decades
- PMID: 31895405
- PMCID: PMC6990848
- DOI: 10.1001/jamaoncol.2019.5582
Life Expectancy of Adult Survivors of Childhood Cancer Over 3 Decades
Abstract
Importance: Advances in childhood and adolescent cancer treatment have been associated with increased rates of cure during the past 3 decades; however, improvement in adult life expectancy for these individuals has not yet been reported.
Objectives: To project long-term survival and assess whether life expectancy will improve among adult survivors of childhood cancer who were treated in more recent decades.
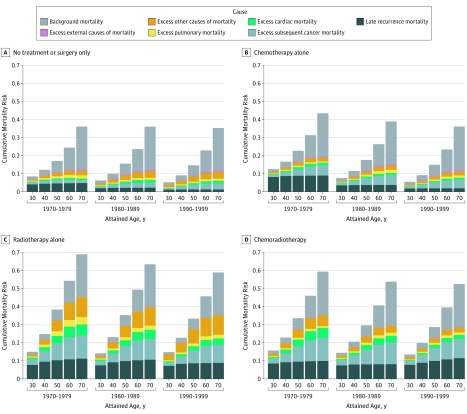
Design, setting, and participants: A microsimulation model of competing mortality risks was developed using data from the Childhood Cancer Survivor Study on 5-year survivors of childhood cancer diagnosed between 1970 and 1999. The model included (1) late recurrence, (2) treatment-related late effects (health-related [subsequent cancers, cardiac events, pulmonary conditions, and other] and external causes), and (3) US background mortality rates.
Exposures: Treatment subgroups (no treatment or surgery only, chemotherapy alone, radiotherapy alone, and radiotherapy with chemotherapy) and individuals with acute lymphoblastic leukemia during childhood by era (1970-1979, 1980-1989, and 1990-1999).
Main outcomes and measures: Conditional life expectancy (defined as the number of years a 5-year survivor can expect to live), cumulative cause-specific mortality risk, and 10-year mortality risks conditional on attaining ages of 30, 40, 50, and 60 years.
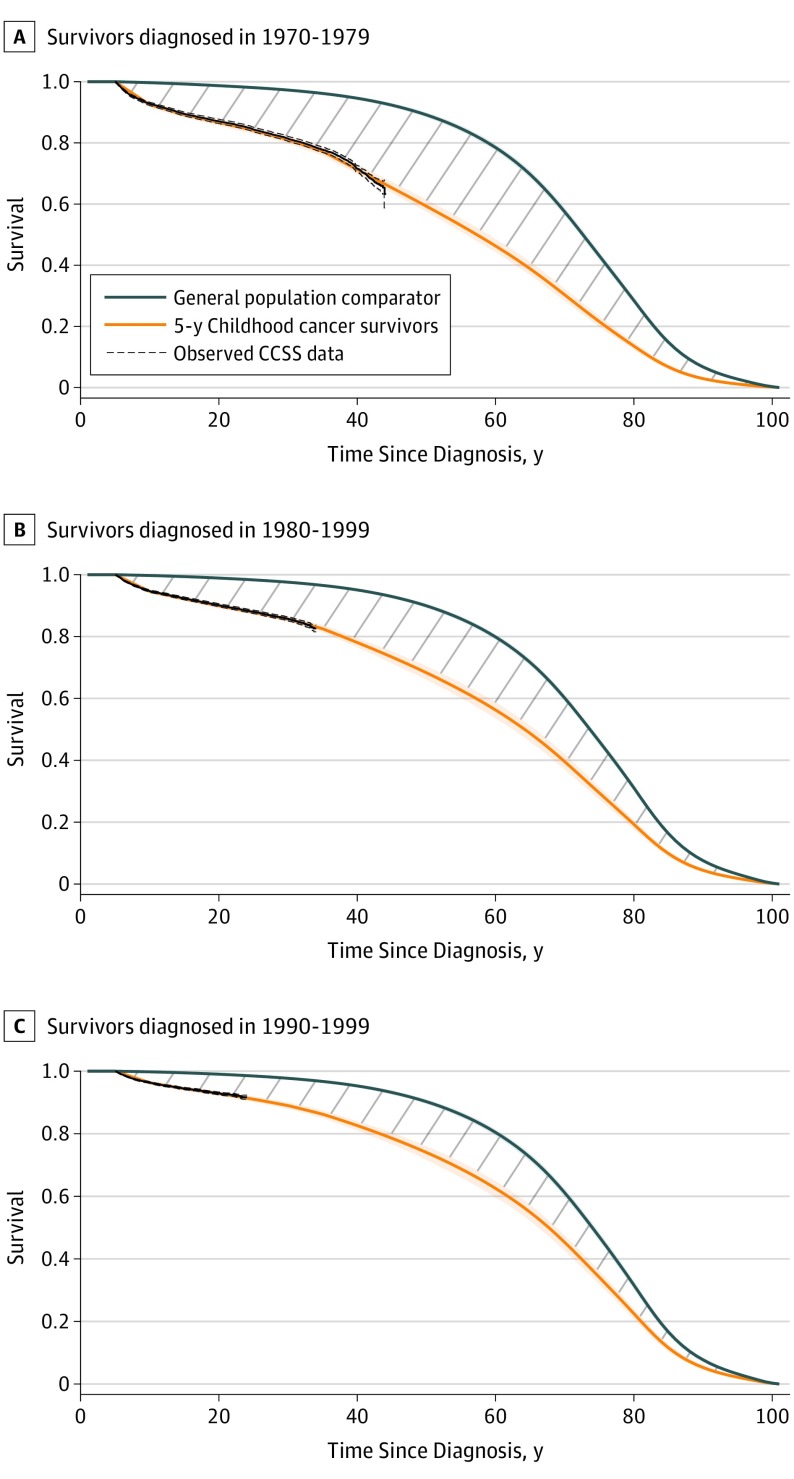
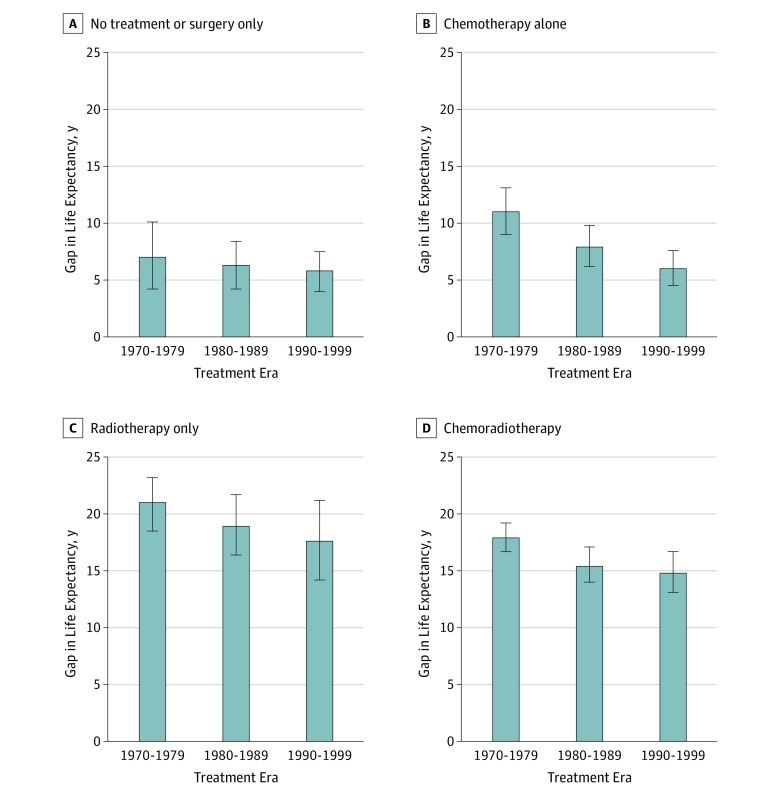
Results: Among the hypothetical cohort of 5-year survivors of childhood cancer representative of the Childhood Cancer Survivor Study participants (44% female and 56% male; mean [SD] age at diagnosis, 7.3 [5.6] years), conditional life expectancy was 48.5 years (95% uncertainty interval [UI], 47.6-49.6 years) for 5-year survivors diagnosed in 1970-1979, 53.7 years (95% UI, 52.6-54.7 years) for those diagnosed in 1980-1989, and 57.1 years (95% UI, 55.9-58.1 years) for those diagnosed in 1990-1999. Compared with individuals without a history of cancer, these results represented a gap in life expectancy of 25% (95% UI, 24%-27%) (16.5 years [95% UI, 15.5-17.5 years]) for those diagnosed in 1970-1979, 19% (95% UI, 17%-20%) (12.3 years [95% UI, 11.3-13.4 years]) for those diagnosed in 1980-1989, and 14% (95% UI, 13%-16%) (9.2 years [95% UI, 8.3-10.4 years]) for those diagnosed in 1990-1999. During the 3 decades, the proportion of survivors treated with chemotherapy alone increased (from 18% in 1970-1979 to 54% in 1990-1999), and the life expectancy gap in this chemotherapy-alone group decreased from 11.0 years (95% UI, 9.0-13.1 years) to 6.0 years (95% UI, 4.5-7.6 years). In contrast, during the same time frame, only modest improvements in the gap in life expectancy were projected for survivors treated with radiotherapy (21.0 years [95% UI, 18.5-23.2 years] to 17.6 years [95% UI, 14.2-21.2 years]) or with radiotherapy and chemotherapy (17.9 years [95% UI, 16.7-19.2 years] to 14.8 years [95% UI, 13.1-16.7 years]). For the largest group of survivors by diagnosis-those with acute lymphoblastic leukemia-the gap in life expectancy decreased from 14.7 years (95% UI, 12.8-16.5 years) in 1970-1979 to 8.0 years (95% UI, 6.2-9.7 years).
Conclusions and relevance: Evolving treatment approaches are projected to be associated with improved life expectancy after treatment for pediatric cancer, in particular among those who received chemotherapy alone for their childhood cancer diagnosis. Despite improvements, survivors remain at risk for shorter lifespans, especially when radiotherapy was included as part of their childhood cancer treatment.
Conflict of interest statement
Figures
Comment in
-
Minding the Gap for Survivors of Childhood Cancer.JAMA Oncol. 2020 Mar 1;6(3):330-332. doi: 10.1001/jamaoncol.2019.5556. JAMA Oncol. 2020. PMID: 31895404 No abstract available.
References
-
- Hewitt M, Greenfield S, Stovall E, eds; National Research Council . From Cancer Patient to Cancer Survivor: Lost in Transition. Washington, DC: National Academies Press; 2005.
-
- Gibson TM, Mostoufi-Moab S, Stratton KL, et al. . Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970-99: a report from the Childhood Cancer Survivor Study cohort. Lancet Oncol. 2018;19(12):1590-1601. doi:10.1016/S1470-2045(18)30537-0 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
