

Palliative Care and End-of-Life Outcomes Following High-risk Surgery
- PMID: 31895424
- PMCID: PMC6990868
- DOI: 10.1001/jamasurg.2019.5083
Palliative Care and End-of-Life Outcomes Following High-risk Surgery
Abstract
Importance: Palliative care has the potential to improve care for patients and families undergoing high-risk surgery.
Objective: To characterize the use of perioperative palliative care and its association with family-reported end-of-life experiences of patients who died within 90 days of a high-risk surgical operation.
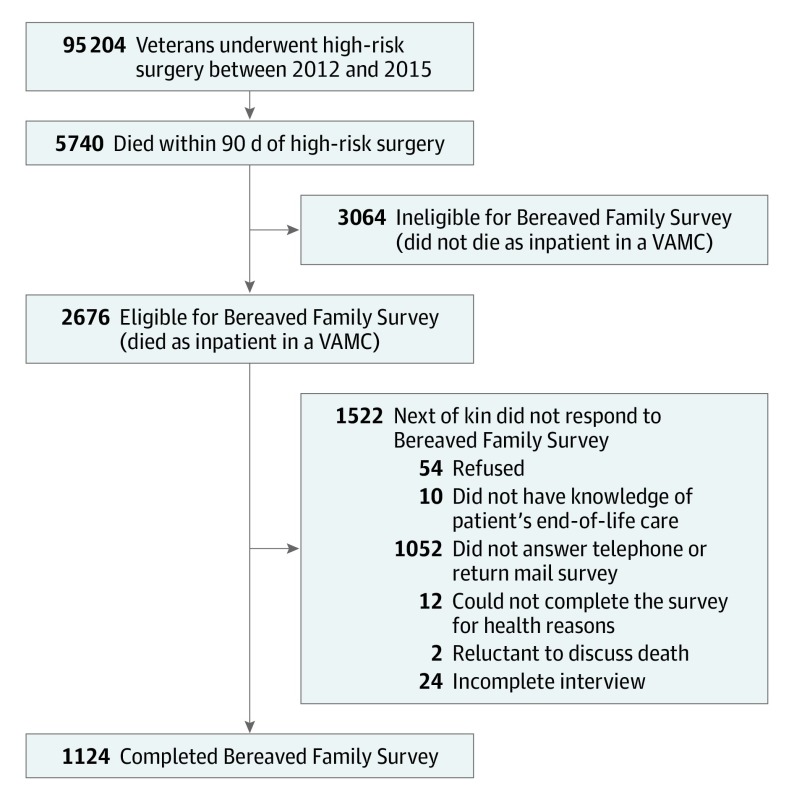
Design, setting, and participants: This secondary analysis of administrative data from a retrospective cross-sectional patient cohort was conducted in the Department of Veterans Affairs (VA) Healthcare System. Patients who underwent any of 227 high-risk operations between January 1, 2012, and December 31, 2015, were included.
Exposures: Palliative-care consultation within 30 days before or 90 days after surgery.
Main outcomes and measures: The outcomes were family-reported ratings of overall care, communication, and support in the patient's last month of life. The VA surveyed all families of inpatient decedents using the Bereaved Family Survey, a valid and reliable tool that measures patient and family-centered end-of-life outcomes.
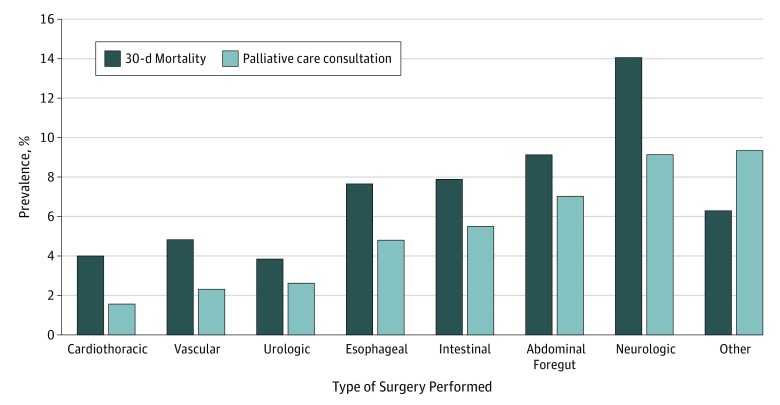
Results: A total of 95 204 patients underwent high-risk operations in 129 inpatient VA Medical Centers. Most patients were 65 years or older (69 278 [72.8%]), and the most common procedures were cardiothoracic (31 157 [32.7%]) or vascular (23 517 [24.7%]). The 90-day mortality rate was 6.0% (5740 patients) and varied by surgical subspecialty (ranging from 278 of 7226 [3.8%] in urologic surgery to 875 of 6223 patients [14.1%] in neurosurgery). A multivariate mixed model revealed that families of decedents who received palliative care were 47% more likely to rate overall care in the last month of life as excellent than those who did not (odds ratio [OR], 1.47 [95% CI, 1.14-1.88]; P = .007), after adjusting for patient's characteristics, surgical subspecialty of the high-risk operation, and survey nonresponse. Similarly, families of decedents who received palliative care were more likely to rate end-of-life communication (OR, 1.43 [95% CI, 1.09-1.87]; P = .004) and support (OR, 1.31 [95% CI, 1.01-1.71]; P = .05) components of medical care as excellent. Of the entire cohort, 3374 patients (3.75%) had a palliative care consultation, and 770 patients (0.8%) received it before surgery. Of all decedents, 1632 (29.9%) had a palliative care consultation, with 319 (5.6%) receiving it before surgery.
Conclusions and relevance: Receipt of a palliative consultation was associated with better ratings of overall end-of-life care, communication, and support, as reported by families of patients who died within 90 days of high-risk surgery. Yet only one-third of decedents was exposed to palliative care. Expanding integration of perioperative palliative care may benefit patients undergoing high-risk operations and their families.
Conflict of interest statement
Figures
Comment in
-
Reimagining Surgical Success-Caring for Those Who Die Despite Our Best Efforts.JAMA Surg. 2020 Feb 1;155(2):146-147. doi: 10.1001/jamasurg.2019.5084. JAMA Surg. 2020. PMID: 31895419 No abstract available.
References
-
- El-Jawahri A, Traeger L, Greer JA, et al. . Effect of inpatient palliative care during hematopoietic stem-cell transplant on psychological distress 6 months after transplant: results of a randomized clinical trial. J Clin Oncol. 2017;35(32):3714-3721. doi:10.1200/JCO.2017.73.2800 - DOI - PMC - PubMed
