

Improved Survival With Extracorporeal Cardiopulmonary Resuscitation Despite Progressive Metabolic Derangement Associated With Prolonged Resuscitation
- PMID: 31896278
- PMCID: PMC7069385
- DOI: 10.1161/CIRCULATIONAHA.119.042173
Improved Survival With Extracorporeal Cardiopulmonary Resuscitation Despite Progressive Metabolic Derangement Associated With Prolonged Resuscitation
Abstract
Background: The likelihood of neurologically favorable survival declines with prolonged resuscitation. However, the ability of extracorporeal cardiopulmonary resuscitation (ECPR) to modulate this decline is unknown. Our aim was to examine the effects of resuscitation duration on survival and metabolic profile in patients who undergo ECPR for refractory ventricular fibrillation/ventricular tachycardia out-of-hospital cardiac arrest.
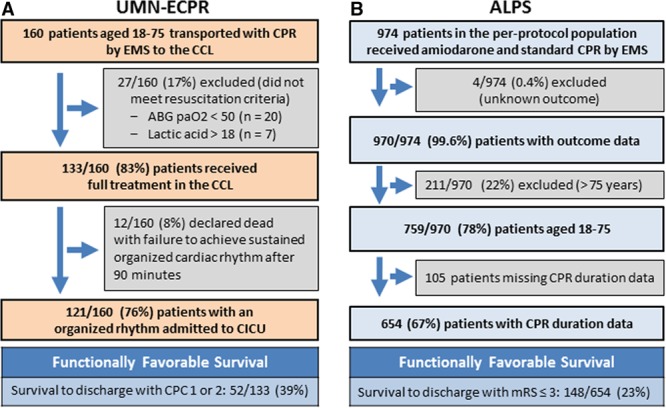
Methods: We retrospectively evaluated survival in 160 consecutive adults with refractory ventricular fibrillation/ventricular tachycardia out-of-hospital cardiac arrest treated with the University of Minnesota (UMN) ECPR protocol (transport with ongoing cardiopulmonary resuscitation [CPR] to the cardiac catheterization laboratory for ECPR) compared with 654 adults who had received standard CPR in the amiodarone arm of the ALPS trial (Amiodarone, Lidocaine, or Placebo Study). We evaluated the metabolic changes and rate of survival in relation to duration of CPR in UMN-ECPR patients.
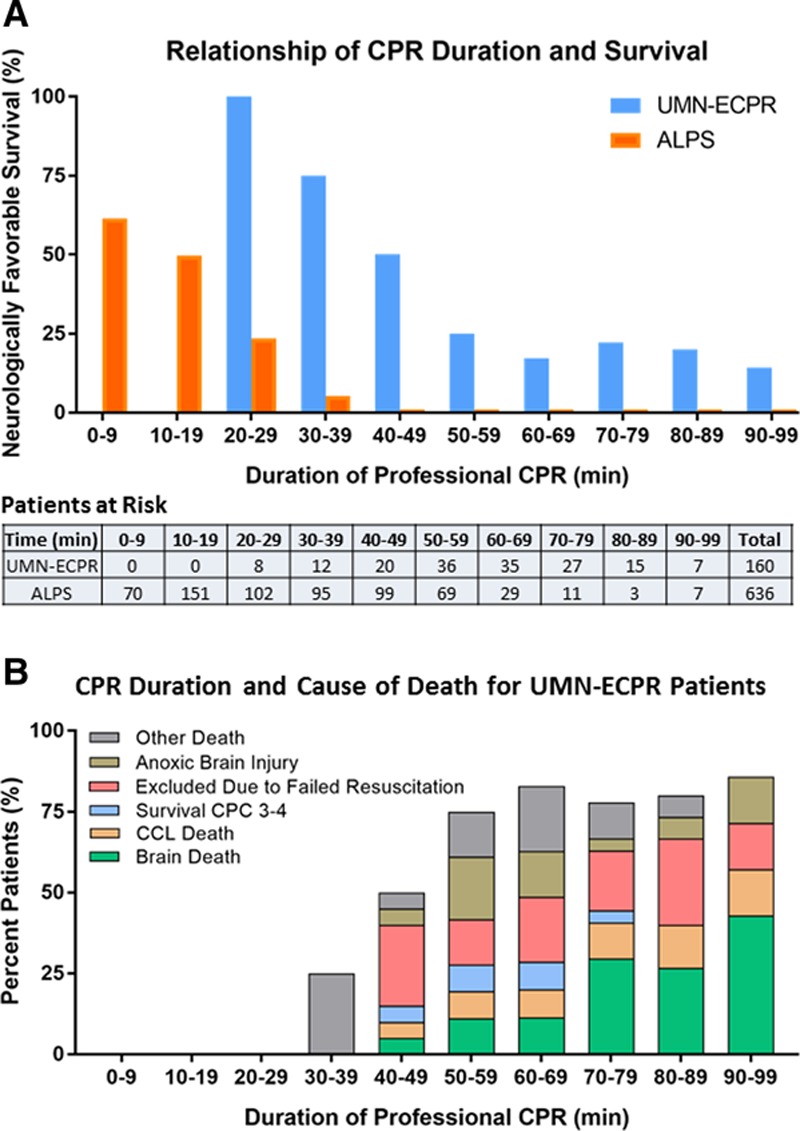
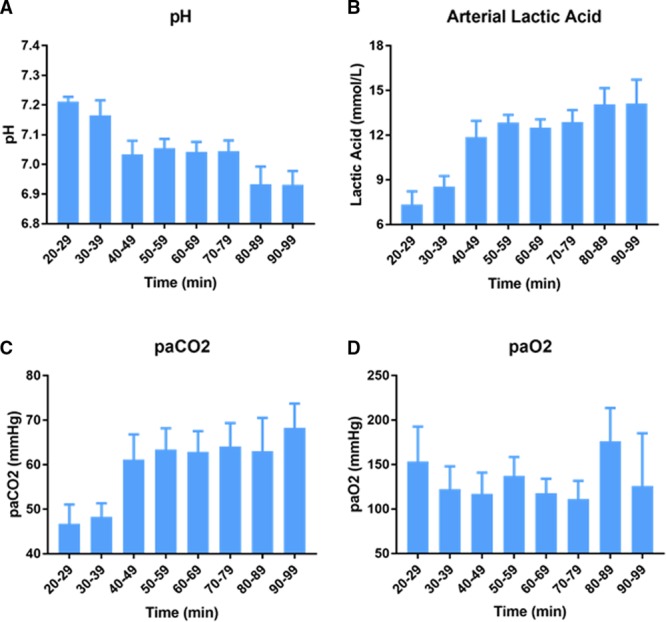
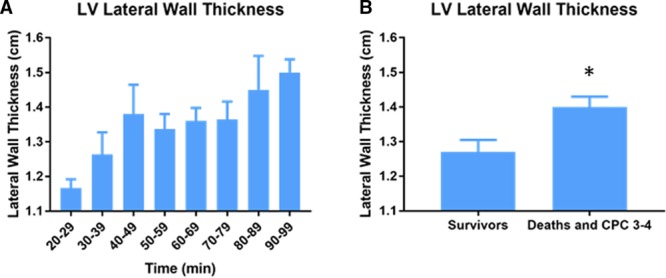
Results: Neurologically favorable survival was significantly higher in UMN-ECPR patients versus ALPS patients (33% versus 23%; P=0.01) overall. The mean duration of CPR was also significantly longer for UMN-ECPR patients versus ALPS patients (60 minutes versus 35 minutes; P<0.001). Analysis of the effect of CPR duration on neurologically favorable survival demonstrated significantly higher neurologically favorable survival for UMN-ECPR patients compared with ALPS patients at each CPR duration interval <60 minutes; however, longer CPR duration was associated with a progressive decline in neurologically favorable survival in both groups. All UMN-ECPR patients with 20 to 29 minutes of CPR (8 of 8) survived with neurologically favorable status compared with 24% (24 of 102) of ALPS patients with the same duration of CPR. There were no neurologically favorable survivors in the ALPS cohort with CPR ≥40 minutes, whereas neurologically favorable survival was 25% (9 of 36) for UMN-ECPR patients with 50 to 59 minutes of CPR and 19% with ≥60 minutes of CPR. Relative risk of mortality or poor neurological function was significantly reduced in UMN-ECPR patients with CPR duration ≥60 minutes. Significant metabolic changes included decline in pH, increased lactic acid and arterial partial pressure of carbon dioxide, and thickened left ventricular wall with prolonged professional CPR.
Conclusions: ECPR was associated with improved neurologically favorable survival at all CPR durations <60 minutes despite severe progressive metabolic derangement. However, CPR duration remains a critical determinate of survival.
Keywords: cardiopulmonary resuscitation; death, sudden, cardiac; extracorporeal membrane oxygenation; heart arrest; ventricular fibrillation.
Figures
Comment in
-
Extracorporeal Cardiopulmonary Resuscitation for Adults With Refractory Out-of-Hospital Cardiac Arrest: Towards Better Neurological Outcomes.Circulation. 2020 Mar 17;141(11):887-890. doi: 10.1161/CIRCULATIONAHA.119.044969. Epub 2020 Mar 16. Circulation. 2020. PMID: 32176540 No abstract available.
-
Letter by den Uil et al Regarding Article, "Improved Survival With Extracorporeal Cardiopulmonary Resuscitation Despite Progressive Metabolic Derangement Associated With Prolonged Resuscitation".Circulation. 2020 Aug 25;142(8):e119-e120. doi: 10.1161/CIRCULATIONAHA.120.046300. Epub 2020 Aug 24. Circulation. 2020. PMID: 32833520 No abstract available.
-
Response by Bartos and Yannopoulos to Letter Regarding Article, "Improved Survival With Extracorporeal Cardiopulmonary Resuscitation Despite Progressive Metabolic Derangement Associated With Prolonged Resuscitation".Circulation. 2020 Aug 25;142(8):e121-e122. doi: 10.1161/CIRCULATIONAHA.120.049328. Epub 2020 Aug 24. Circulation. 2020. PMID: 32833521 No abstract available.
References
-
- Becker LB, Aufderheide TP, Graham R. Strategies to improve survival from cardiac arrest: a report from the Institute of Medicine. JAMA. 2015;314:223–224. doi: 10.1001/jama.2015.8454. - PubMed
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2019 update: a report from the American Heart Association. Circulation. 2019;139:e56–e528. doi: 10.1161/CIR.0000000000000659. - PubMed
-
- Aufderheide TP, Frascone RJ, Wayne MA, Mahoney BD, Swor RA, Domeier RM, Olinger ML, Holcomb RG, Tupper DE, Yannopoulos D, et al. Standard cardiopulmonary resuscitation versus active compression-decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out-of-hospital cardiac arrest: a randomised trial. Lancet. 2011;377:301–311. doi: 10.1016/S0140-6736(10)62103-4. - PMC - PubMed
-
- Aufderheide TP, Nichol G, Rea TD, Brown SP, Leroux BG, Pepe PE, Kudenchuk PJ, Christenson J, Daya MR, Dorian P, et al. Resuscitation Outcomes Consortium (ROC) Investigators. A trial of an impedance threshold device in out-of-hospital cardiac arrest. N Engl J Med. 2011;365:798–806. doi: 10.1056/NEJMoa1010821. - PMC - PubMed
-
- Dumas F, Bougouin W, Geri G, Lamhaut L, Rosencher J, Pene F, Chiche JD, Varenne O, Carli P, Jouven X, et al. Emergency percutaneous coronary intervention in post-cardiac arrest patients without ST-segment elevation pattern: insights from the PROCAT II registry. JACC Cardiovasc Interv. 2016;9:1011–1018. doi: 10.1016/j.jcin.2016.02.001. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
