

Distinct Growth Phases in Early Life Associated With the Risk of Type 1 Diabetes: The TEDDY Study
- PMID: 31896601
- PMCID: PMC7035588
- DOI: 10.2337/dc19-1670
Distinct Growth Phases in Early Life Associated With the Risk of Type 1 Diabetes: The TEDDY Study
Abstract
Objective: This study investigates two-phase growth patterns in early life and their association with development of islet autoimmunity (IA) and type 1 diabetes (T1D).
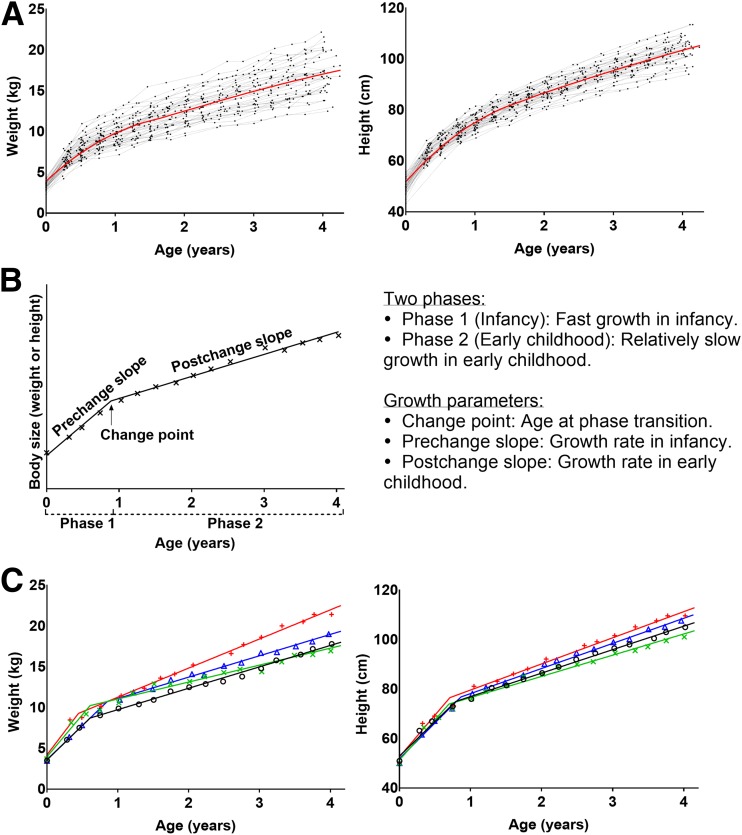
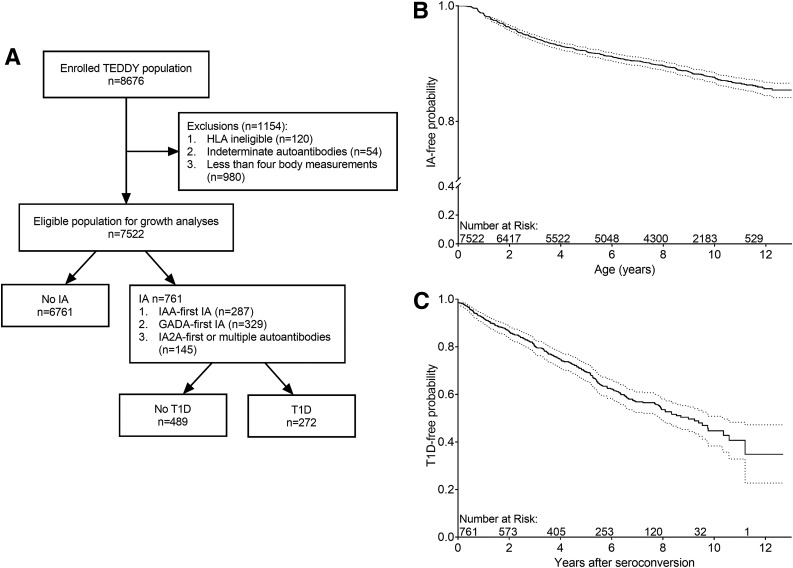
Research design and methods: The Environmental Determinants of Diabetes in the Young (TEDDY) study followed 7,522 genetically high-risk children in Sweden, Finland, Germany, and the U.S. from birth for a median of 9.0 years (interquartile range 5.7-10.6) with available growth data. Of these, 761 (10.1%) children developed IA and 290 (3.9%) children were diagnosed with T1D. Bayesian two-phase piecewise linear mixed models with a random change point were used to estimate children's individual growth trajectories. Cox proportional hazards models were used to assess the effects of associated growth parameters on the risks of IA and progression to T1D.
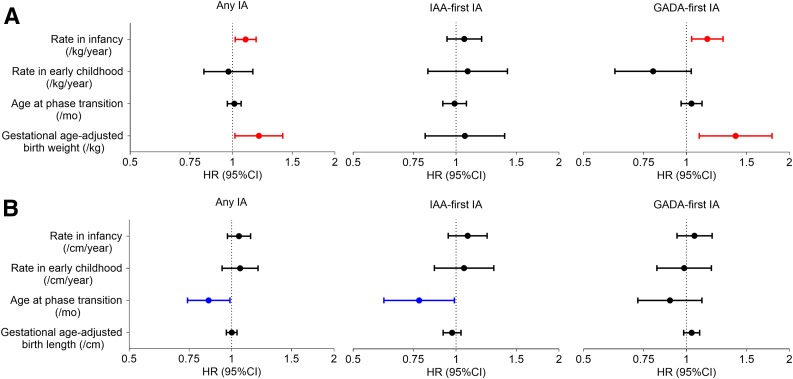
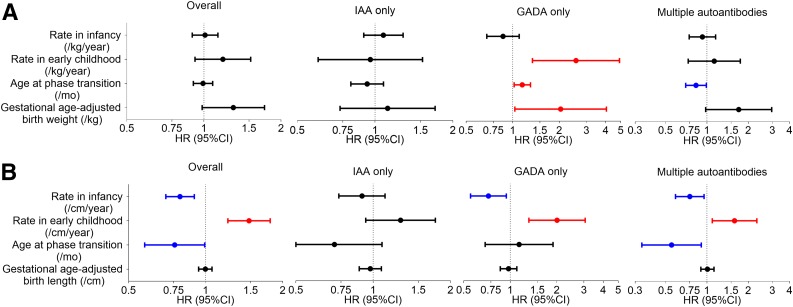
Results: A higher rate of weight gain in infancy was associated with increased IA risk (hazard ratio [HR] 1.09 [95% CI 1.02, 1.17] per 1 kg/year). A height growth pattern with a lower rate in infancy (HR 0.79 [95% CI 0.70, 0.90] per 1 cm/year), higher rate in early childhood (HR 1.48 [95% CI 1.22, 1.79] per 1 cm/year), and younger age at the phase transition (HR 0.76 [95% CI 0.58, 0.99] per 1 month) was associated with increased risk of progression from IA to T1D. A higher rate of weight gain in early childhood was associated with increased risk of progression from IA to T1D (HR 2.57 [95% CI 1.34, 4.91] per 1 kg/year) in children with first-appearing GAD autoantibody only.
Conclusions: Growth patterns in early life better clarify how specific growth phases are associated with the development of T1D.
© 2020 by the American Diabetes Association.
Figures
References
-
- Vehik K, Dabelea D. The changing epidemiology of type 1 diabetes: why is it going through the roof? Diabetes Metab Res Rev 2011;27:3–13 - PubMed
-
- Knip M, Veijola R, Virtanen SM, Hyöty H, Vaarala O, Åkerblom HK. Environmental triggers and determinants of type 1 diabetes. Diabetes 2005;54(Suppl. 2):S125–S136 - PubMed
-
- Wilkin TJ. The accelerator hypothesis: weight gain as the missing link between type I and type II diabetes. Diabetologia 2001;44:914–922 - PubMed
-
- Dahlquist G. Can we slow the rising incidence of childhood-onset autoimmune diabetes? The overload hypothesis. Diabetologia 2006;49:20–24 - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK063821/DK/NIDDK NIH HHS/United States
- UC4 DK063863/DK/NIDDK NIH HHS/United States
- HHSN267200700014C/DK/NIDDK NIH HHS/United States
- U01 DK063861/DK/NIDDK NIH HHS/United States
- U01 DK063790/DK/NIDDK NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- U01 DK063836/DK/NIDDK NIH HHS/United States
- U01 DK063829/DK/NIDDK NIH HHS/United States
- U01 DK063865/DK/NIDDK NIH HHS/United States
- UC4 DK095300/DK/NIDDK NIH HHS/United States
- UC4 DK063861/DK/NIDDK NIH HHS/United States
- UC4 DK063829/DK/NIDDK NIH HHS/United States
- UC4 DK063821/DK/NIDDK NIH HHS/United States
- UC4 DK117483/DK/NIDDK NIH HHS/United States
- UC4 DK063836/DK/NIDDK NIH HHS/United States
- UC4 DK112243/DK/NIDDK NIH HHS/United States
- UC4 DK063865/DK/NIDDK NIH HHS/United States
- U01 DK063863/DK/NIDDK NIH HHS/United States
- UC4 DK106955/DK/NIDDK NIH HHS/United States
- UC4 DK100238/DK/NIDDK NIH HHS/United States
