

Incorporation of differentiated dysplasia improves prediction of oral leukoplakia at increased risk of malignant progression
- PMID: 31896811
- PMCID: PMC7280084
- DOI: 10.1038/s41379-019-0444-0
Incorporation of differentiated dysplasia improves prediction of oral leukoplakia at increased risk of malignant progression
Abstract
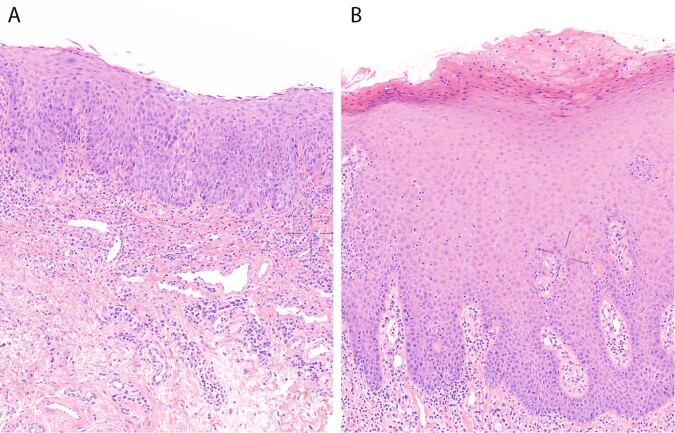
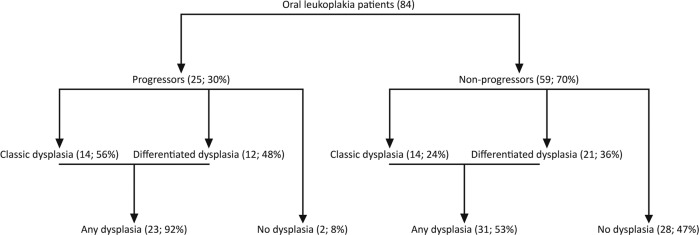
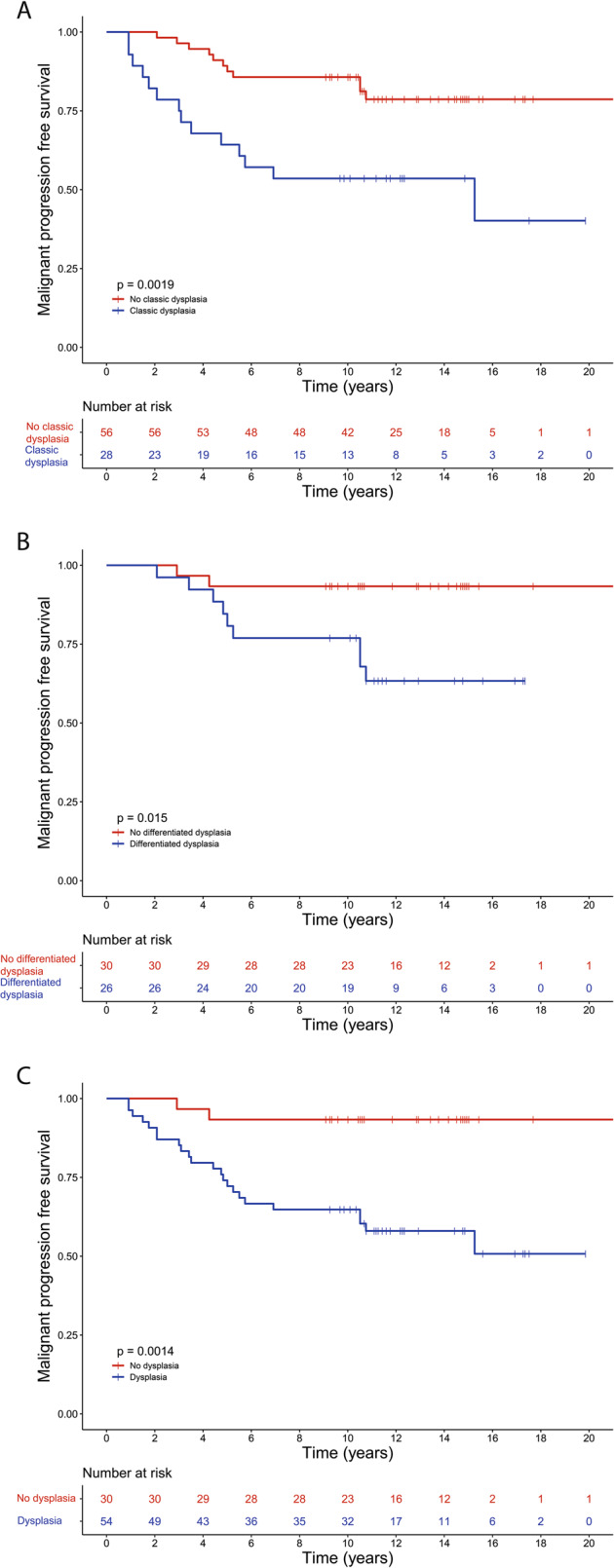
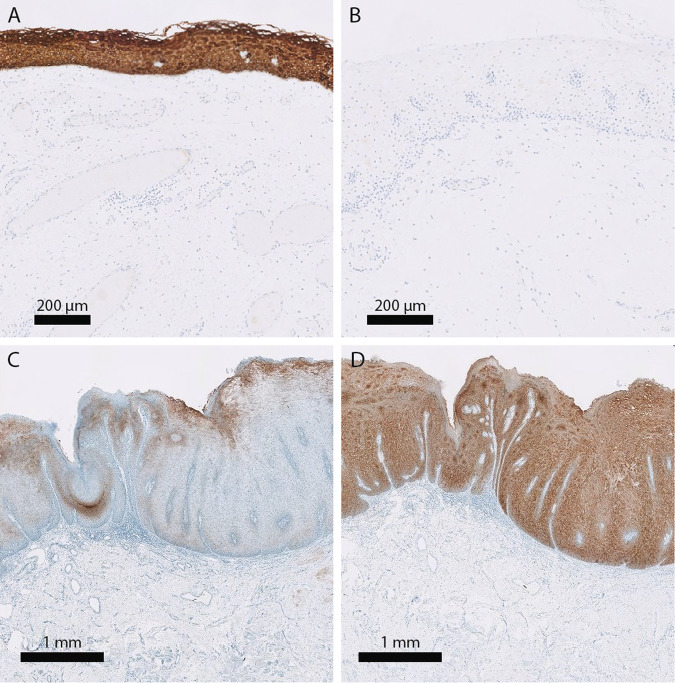
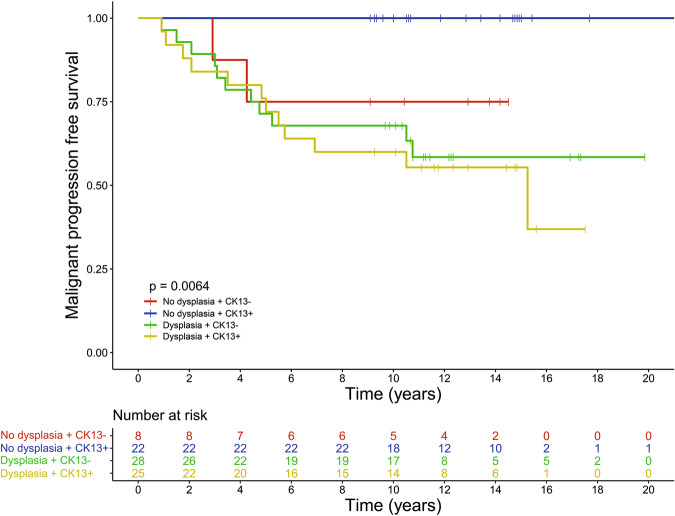
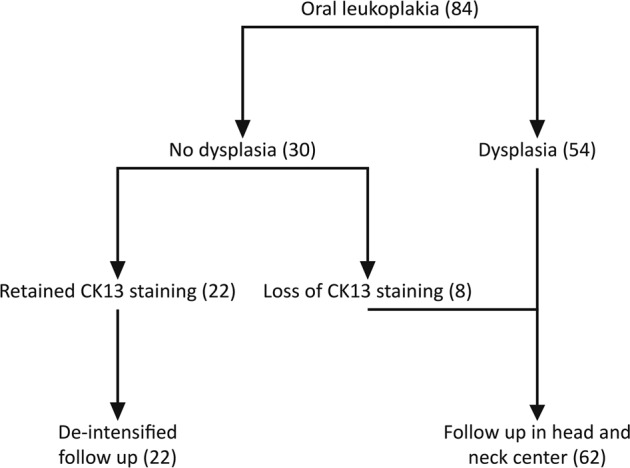
Oral leukoplakia is the most common oral potentially malignant disorder with a malignant transformation rate into oral squamous cell carcinoma of 1-3% annually. The presence and grade of World Health Organization defined dysplasia is an important histological marker to assess the risk for malignant transformation, but is not sufficiently accurate to personalize treatment and surveillance. Differentiated dysplasia, known from differentiated vulvar intraepithelial neoplasia, is hitherto not used in oral dysplasia grading. We hypothesized that assessing differentiated dysplasia besides World Health Organization defined (classic) dysplasia will improve risk assessment of malignant transformation of oral leukoplakia. We investigated a retrospective cohort consisting of 84 oral leukoplakia patients. Biopsies were assessed for dysplasia presence and grade, and the expression of keratins 13 (CK13) and 17, known to be dysregulated in dysplastic vulvar mucosa. In dysplastic oral lesions, differentiated dysplasia is as common as classic dysplasia. In 25 out of 84 (30%) patients, squamous cell carcinoma of the upper aerodigestive tract developed during follow-up. Considering only classic dysplasia, 11 out of 56 (20%) patients with nondysplastic lesions progressed. With the incorporation of differentiated dysplasia, only 2 out of 30 (7%) patients with nondysplastic lesions progressed. The risk of progression increased from 3.26 (Hazard ratio, p = 0.002) when only classic dysplasia is considered to 7.43 (Hazard ratio, p = 0.001) when classic and differentiated dysplasia are combined. Loss of CK13, combined with presence of dysplasia, is associated with greater risk of malignant progression (p = 0.006). This study demonstrates that differentiated dysplasia should be recognized as a separate type of dysplasia in the oral mucosa and that its distinction from classic dysplasia is of pathological and clinical significance since it is a strong (co)prognostic histopathological marker for oral malignant transformation. In oral lesions without dysplasia and retained CK13 staining the risk for progression is very low.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
The role of differentiated dysplasia in the prediction of malignant transformation of oral leukoplakia.J Oral Pathol Med. 2023 Nov;52(10):930-938. doi: 10.1111/jop.13483. Epub 2023 Sep 25. J Oral Pathol Med. 2023. PMID: 37749621
-
[Identification of differentiated dysplasia improves prediction of oral leukoplakia at increased risk of malignant progression].Ned Tijdschr Tandheelkd. 2021 Feb;128(2):103-111. doi: 10.5177/ntvt.2021.02.20078. Ned Tijdschr Tandheelkd. 2021. PMID: 33605260 Dutch.
-
Diagnosis of differentiated dysplasia as a variant of oral epithelial dysplasia.Oral Dis. 2024 Oct;30(7):4185-4194. doi: 10.1111/odi.14846. Epub 2024 Jan 8. Oral Dis. 2024. PMID: 38191851
-
Oral premalignant lesions: from a clinical perspective.Int J Clin Oncol. 2011 Feb;16(1):5-14. doi: 10.1007/s10147-010-0157-3. Epub 2011 Jan 12. Int J Clin Oncol. 2011. PMID: 21225307 Review.
-
[Oral medicine 8. Leukoplakia of the oral mucosa].Ned Tijdschr Tandheelkd. 2013 Jul-Aug;120(7-8):384-90. Ned Tijdschr Tandheelkd. 2013. PMID: 23923441 Review. Dutch.
Cited by
-
Oral cancer prediction by noninvasive genetic screening.Int J Cancer. 2023 Jan 15;152(2):227-238. doi: 10.1002/ijc.34277. Epub 2022 Sep 18. Int J Cancer. 2023. PMID: 36069231 Free PMC article.
-
Resection Margins in Head and Neck Cancer Surgery: An Update of Residual Disease and Field Cancerization.Cancers (Basel). 2021 May 27;13(11):2635. doi: 10.3390/cancers13112635. Cancers (Basel). 2021. PMID: 34071997 Free PMC article. Review.
-
Immunohistochemical staining patterns of p53 predict the mutational status of TP53 in oral epithelial dysplasia.Mod Pathol. 2022 Feb;35(2):177-185. doi: 10.1038/s41379-021-00893-9. Epub 2021 Aug 17. Mod Pathol. 2022. PMID: 34404905
-
[Progress in clinicopathological diagnosis of oral potentially malignant disorders].Hua Xi Kou Qiang Yi Xue Za Zhi. 2025 Jun 1;43(3):314-324. doi: 10.7518/hxkq.2025.2024427. Hua Xi Kou Qiang Yi Xue Za Zhi. 2025. PMID: 40523811 Free PMC article. Review. Chinese.
-
New insights into the role of the oral leukoplakia microenvironment in malignant transformation.Front Oral Health. 2024 Feb 21;5:1363052. doi: 10.3389/froh.2024.1363052. eCollection 2024. Front Oral Health. 2024. PMID: 38450102 Free PMC article. Review.
References
-
- Reibel J, Gale N, Hille J, Hunt JL, Lingen M, Muller S, et al. Tumours of the oral cavity and mobile tongue. In: El-Naggar AK, Chan JKC, Grandis JR, et al. editors. WHO classification of head and neck tumours, 4th ed. Lyon: IARC press; 2017. p. 112–4.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
