

Clinical Implications of Microsatellite Instability in Early Gastric Cancer
- PMID: 31897345
- PMCID: PMC6928080
- DOI: 10.5230/jgc.2019.19.e38
Clinical Implications of Microsatellite Instability in Early Gastric Cancer
Abstract
Purpose: We aimed to evaluate the clinical characteristics of microsatellite instability in early gastric cancer.
Materials and methods: The microsatellite instability status of resected early gastric tumors was evaluated using two mononucleotide repeat markers (BAT25 and BAT26) and three dinucleotide repeat markers (D5S346, D2S123, and D17S250). Tumors with instability in two or more markers were defined as microsatellite instability-high (MSI-H) and others were classified as microsatellite stable (MSS).
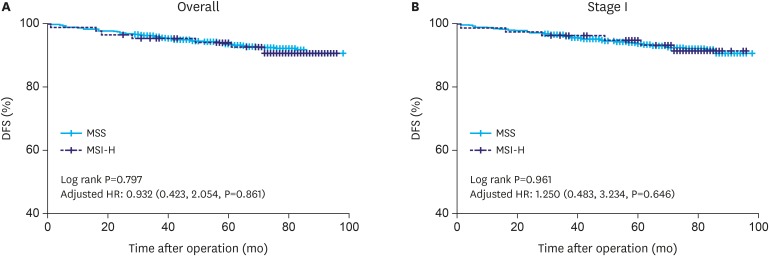
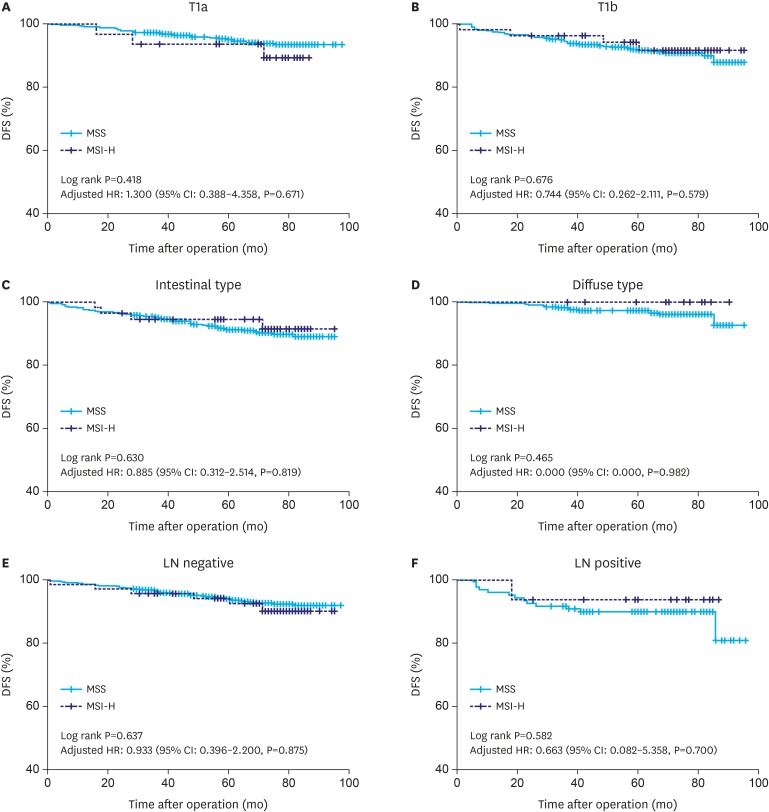
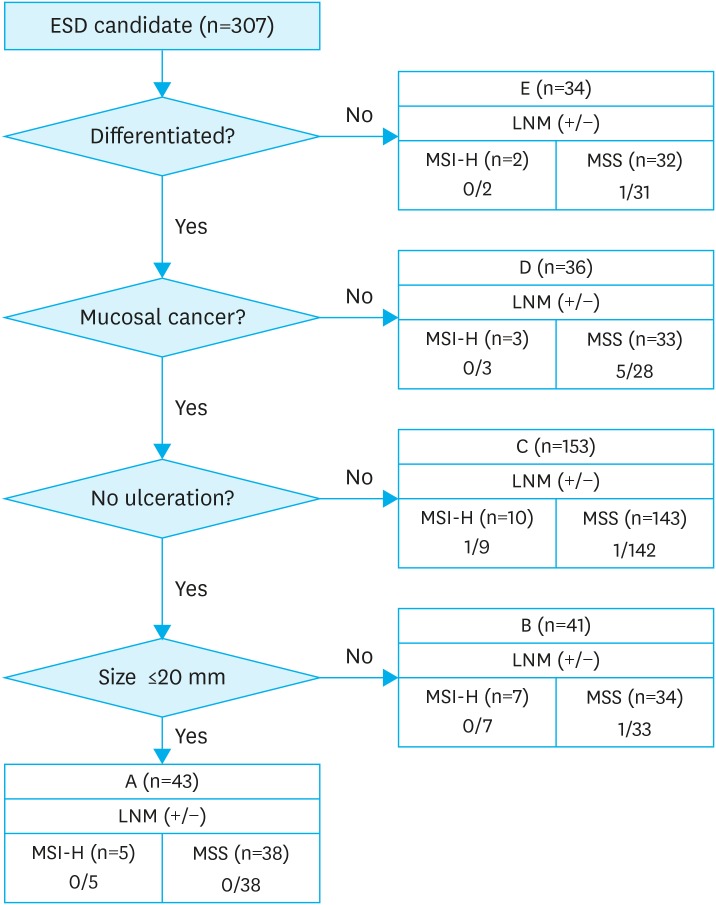
Results: Overall, 1,156 tumors were included in the analysis, with 85 (7.4%) classified as MSI-H compared with MSS tumors. For MSI-H tumors, there was a significant correlation with the female sex, older age, tumor location in the lower gastric body, intestinal histology, lymphovascular invasion (LVI), and submucosal invasion (P<0.05). There was also a trend toward an association with lymph node (LN) metastasis (P=0.056). In mucosal gastric cancer, there was no significant difference in MSI status in tumors with LN metastasis or tumors with LVI. In submucosal gastric cancer, LVI was more frequently observed in MSI-H than in MSS tumors (38.9% vs. 25.0%, P=0.027), but there was no difference in the presence of LN metastases. The prognosis of MSI-H tumors was similar to that of MSS tumors (log-rank test, P=0.797, the hazard ratio for MSI-H was adjusted by age, sex, pT stage, and the number of metastatic LNs, 0.932; 95% confidence interval, 0.423-2.054; P=0.861).
Conclusions: MSI status was not useful in predicting prognosis in early gastric cancer. However, the frequent presence of LVI in early MSI-H gastric cancer may help guide the appropriate treatment for patients, such as endoscopic treatment or limited LN surgical dissection.
Keywords: Gastric cancer; Lymph nodes; Microsatellite instability; Prognosis.
Copyright © 2019. Korean Gastric Cancer Association.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Sugano K. Screening of gastric cancer in Asia. Best Pract Res Clin Gastroenterol. 2015;29:895–905. - PubMed
-
- Lai JF, Kim S, Kim K, Li C, Oh SJ, Hyung WJ, et al. Prediction of recurrence of early gastric cancer after curative resection. Ann Surg Oncol. 2009;16:1896–1902. - PubMed
LinkOut - more resources
Full Text Sources
