

Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
- PMID: 31897434
- PMCID: PMC6920588
- DOI: 10.1177/2382120519894270
Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Abstract
Background: Clinicians are key drivers for improving health care quality and safety. However, some may lack experience in quality improvement and patient safety (QI/PS) methodologies, including root cause analysis (RCA).
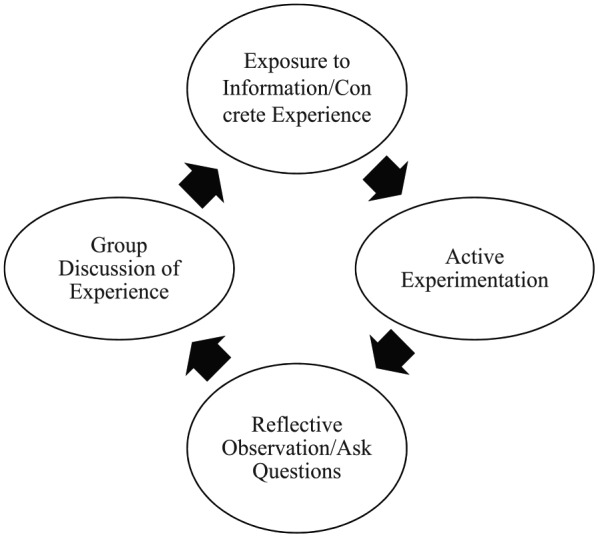
Objective: The Department of Veterans Affairs (VA) sought to develop a simulation approach to teach clinicians from the VA's Chief Resident in Quality and Safety program about RCA. We report the use of experiential learning to teach RCA, and clinicians' preparedness to conduct and teach RCA post-training. We provide curriculum details and materials to be adapted for widespread use.
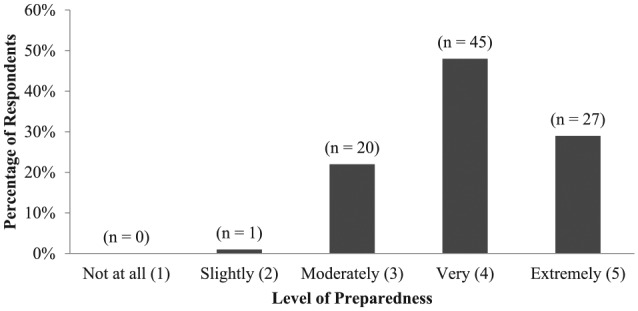
Methods: The course was designed to meet the learning objectives through simulation. We developed course materials, including presentations, a role-playing case, and an elaborate RCA case. Learning objectives included (1) basic structure of RCA, (2) process flow diagramming, (3) collecting information for RCA, (4) cause and effect diagramming, and (5) identifying actions and outcomes. We administered a voluntary, web-based survey in November 2016 to participants (N = 114) post-training to assess their competency with RCA.
Results: A total of 93 individuals completed the survey of the 114 invited to participate, culminating an 82% response rate. Nearly all respondents (99%, N = 92) reported feeling at least moderately to extremely prepared to conduct and teach RCA post-training. Most respondents reported feeling very to extremely prepared to conduct and teach RCA (77%, N = 72).
Conclusions: Experiential learning involving simulations may be effective to improve clinicians' competency in QI/PS practices, including RCA. Further research is warranted to understand how the training affects clinicians' capacity to participate in real RCA teams post-training, as well as applicability to other disciplines and interdisciplinary teams.
Keywords: curriculum; medical education; patient safety; quality improvement; root cause analysis; simulation.
© The Author(s) 2019.
Conflict of interest statement
Declaration of Conflicting Interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Institute of Medicine Committee on Quality of Health Care in A. In: Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000;17-158. - PubMed
-
- Aboumrad M, Fuld A, Soncrant C, Neily J, Paull D, Watts BV. Root cause analysis of oncology adverse events in the Veterans Health Administration. J Oncol Pract. 2018;14:e579-e590. - PubMed
-
- Neily J, Mills PD, Paull DE, et al. Sharing lessons learned to prevent incorrect surgery. Am Surg. 2012;78:1276-1280. - PubMed
-
- Weingart SN, Price J, Duncombe D, et al. Patient-reported safety and quality of care in outpatient oncology. Jt Comm J Qual Patient Saf. 2007;33:83-94. - PubMed
LinkOut - more resources
Full Text Sources
